|
|
|
|
|
|

|
|
|
|
|
|
 |
|
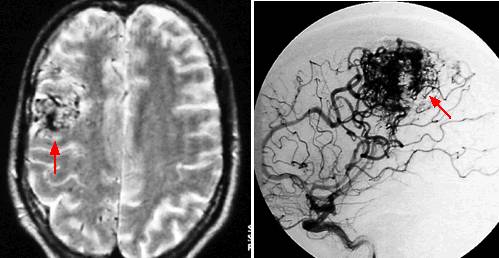
| Radiosurgery works by inducing an injury response in the AVM nidus and
obliterating the vascular tumor in 60-90% of the cases. MRI 's reveal postOp changes in
30% of the patients but 2/3 of these are asymptomatic and only 9% of all patients suffer
complications. (Pitt) (Other data suggests obliteration rate of ~ 80% but lower for large
lesions (77% 10-15ccc and 25% > 155cc from Pan.) Complication rates in literature 2 -5%
and 7 - 9 %.
In the study from Pitt on 832 cases had an obliteration rate of 72%, with 6% complications., based on volume they report the following rates of obliterating the entire AVM or at least the target volume: (also note importance of dose, takes 20Gy to get to 80% success rate.) |
| Volume | Obliterate AVM | Obliterate Target |
| < 1.3cc | 90% | 98% |
| 1.4 - 3cc | 84% | 96% |
| 3 - 5.5cc | 71% | 90% |
| 5.5 - 18cc | 41% | 76% |
| Single doses of radiation
delivered by stereotactic radiosurgical technology (and dose prescriptions of the order of
2000cGy marginal dose), obliterate approximately 75-80% of small (<2.5 cm) AVM and 50%
of 3 cm AVM. Dose guidelines are 2000-2500 cGy to the perimeter of the nidus for lesions less than 2.5 cm and in brain areas not deemed extra sensitive. Extra sensitive sited lesions will receive at least 10-25% dose reductions. The optic chiasm should not receive more than 800-900 cGy in a single fraction and the majority diameter of the brainstem no more than 1250 cGy (whole diameter probably as for optic chiasm). Thus for cases involving the brainstem it would be usual to prescribe of the order of 1250-1500 cGy on the perimeter such that the above normal tissue dose tolerance planning limitations are not exceeded. |
![]()

{kind=link}