|
|
|
|
|
|
 |
Pet scan showing a sarcoma in the leg that has spread to the lymph node |
Some cancers produce chemicals that can be measured in the blood (notably PSA for prostate cancer and CA-125 for ovarian cancer) called tumor markers. Many cancers do not produce such markers and so blood tests may not reveal cancer. (see section on tumor markers and PSA.)
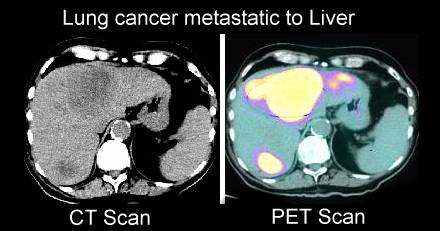
X-rays or imaging studies can often identify the extent and sites of spread of cancers, but there are also limitations (many breast cancers in young women will not be visible on mammograms and lung cancers are hard to identify early on conventional chest X-rays. Imaging has come a long way in the past century (see here, here and here). PET scans have been a significant improvement for many sites of cancer. (see sections on brain imaging, PET scans, mammograms/breast MRI and, lung imaging.)
Details on diagnostic studies are described in the section on anatomy and imaging.
Despite high levels of tumor markers or clearly malignant appearing cancers on X-rays or PET scans a biopsy is still often necessary to be 100% sure of the diagnosis of cancer. Exceptions can be made when attempts to get a tissue diagnosis are too risky (e.g. deep brain tumors or hard to reach lung lesions.)
{kind=link}
{kind=link}
{kind=link}