|
|
|
|
|
|
|
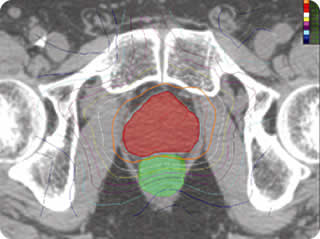
Cyberknife and Prostate Cancer
Some on going clinical trials are listed here, and here using doses like 7.25Gy X 5 (Seattle) or 9.5Gy X 4 (San Diego). The technique form Katz (New York) for low risk patients (7.25Gy X
5) to gland plus 5mm margins (3mm rectum) and 2 cuts of seminal vesicles with rectal
amifostine or as a boost after pelvis XRT in high risk patients (7Gy X 3)
(see data here). |

| CyberKnife radiotherapy for localized prostate cancer:
rationale and technical feasibility. (GO HERE) King CR, Lehmann J, Adler JR, Hai J. Technol Cancer Res Treat. 2003 Feb;2(1):25-30. Department of Radiation Oncology, Stanford University School of Medicine There is a clear dose response for localized prostate cancer radiotherapy and there probably is a radiobiological rationale for hypo-fractionation. Combining the two should maximize tumor control and increase the therapeutic ratio. This study examines the rationale and technical feasibility of CyberKnife radiotherapy (a robotic arm-driven linear accelerator) for localized prostate cancer. Its ability to deliver non-coplanar non-isocentric arcs can yield maximally conformal isodoses. |
|
It is the only integrated system capable of target
position verification and real-time tracking during delivery of conformal stereotactic
radiotherapy. Inverse planning with the CyberKnife is used to design a course of
radiotherapy for localized prostate cancer. Fiducial markers within the gland are used to
verify organ position and track organ motion via an orthogonal pair of electronic x-ray
imaging devices and provide real-time feedback correction to the robotic arm during
delivery. Conformal isodose curves and dose volume histograms (DVH) are used to compare
with an optimized Intensity-Modulated Radiotherapy (IMRT) plan actually delivered to the
study patient based upon CT scan-derived organ volumes. The CyberKnife can produce
superior DVHs for sparing of rectum and bladder and excellent DVHs for target coverage
compared with IMRT, and possesses dose heterogeneities to the same degree as IMRT
plans. Because of the significantly longer delivery times required it would be best suited
for hypo-fractionated regimens. Such dose regimens might allow for biologically equivalent
dose escalation without increased normal tissue toxicity. Since the CyberKnife can verify
organ position and motion and correct for this in real-time it is the ideal means of
achieving such excellent DVHs without a compromise in doses to normal tissues. These
capabilities are essential if one contemplates hypo-fractionated regimens with large
dose-per-fraction sizes (>5Gy to 10Gy) and dose-escalation.
