|
|
|
|
|
|
|
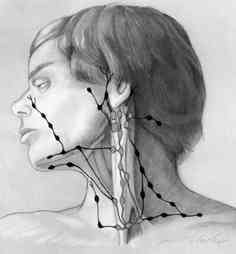
The lymph nodes in the
neck (called cervical nodes) are common sites of spread from
cancers in the head and neck area. The staging system (1983 AJCC) was as follows:
|
|
|
|
|
|
|
|
The lymph nodes in the
neck (called cervical nodes) are common sites of spread from
cancers in the head and neck area. The staging system (1983 AJCC) was as follows:
|
| The treatment of metastatic cancer in the lymph nodes is related to the type of cancer and the size of the nodes. Some node cancers (e.g. lymphoma) are very sensitive to radiation (or chemotherapy) and surgery is not indicated. Most head and neck cancers are squamous cell carcinomas and for large nodes surgery is necessary (except nasopharynx cancer where surgery is less often used.) For patients with multiple nodes chemotherapy probably plays an increasing role. In general a small single node up to 2-3 cm (so called N1) can be treated adequately with surgery (usually a radical neck dissection) or radiation. Larger nodes or multiple nodes (N2 or N3) usually require combined surgery and radiation. In the past surgery was always a radical neck dissection but there has been increasing use of more limited resections. Also some nodes (e.g. retropharyngeal nodes) cannot be resected and radiation is always indicated. The risk of spread to these nodes is noted below: |
| Primary Site | Risk of Node Spread |
| nasopharynx | 74% |
| pharyngeal wall | 19% |
| soft palate | 13% |
| tonsillar region | 9% |
| pyriform/ postcricoid | 5% |
| base of tongue | 4% |
| supraglottic larynx | 2% |
![]()
![]()
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}