 |
Candidates for seed implantation depend on a number of considerations: also see the American Brachytherapy Society (ABS)
Recommendations for Prostate Seed Implants |
|
Candidates for seed implantation depend on a number of considerations: also see the American Brachytherapy Society (ABS)
Recommendations for Prostate Seed Implants |
1. local anatomy - the gland should not be too large (> 50 - 60 ml, the normal prostate gland is about 30ml, go here), should not have a large TURP defect, or the malignant nodule located in an area difficult to implant. the success of the implant depends on an even distribution of the seeds (otherwise it is safer to combine the implant with external beam radiation which will even out the "hot spots and cold spots") 2. risk of regional spread - from Partin Data, PSA > 10. GS > 6 or stage > T2a, or high risk path findings (e.g. vascular invasion or diffuse disease) all increase risk of some regional spread and the need for combing the seeds with external beam irradiation (EBT) 3. risk of distant spread - patient at high risk for distant metastases (GS 8 or higher or PSA > 15-20) would be candidates for systemic therapy (i.e. hormonal therapy e.g. Lupron +/- Casodex or Flutamide) (note that the results with implants alone are poor in higher risk groups, see results page.) |
| Category | Implant | External Beam | Hormones |
| Low Risk | 145Gy I-125 or 125Gy Pd 103 | None | None |
| Medium Risk | 110Gy I-125 or 100Gy Pd 103 | 45Gy | Yes or No |
| High Risk | 110Gy I-125 or 100Gy Pd 103 | 45Gy | Yes |
| Low Risk = favorable
anatomy, PSA < 10, GS 6 or less, stage T1c or T2a, no adverse pathologic findings (no
perineural invasion and tumor confined to one lobe.) some would
restrict low risk to
Gleason score of 6 or less as in RTOG below Medium Risk = PSA > 10 or GS 7 or higher, stage > T2a, unfavorable local anatomy, high risk path report High Risk = Gleason Score of 8 or higher, PSA > 20 Note: there is still controversy over the merits of Palladium versus Iodine. Also
combining therapy can increase the risk of complications, particularly impotence as noted:
risk of impotence with seeds alone (~ 20%) with seeds + external beam (~ 25 - 30%) and
with seeds + hormones (=/- external beam, risk is ~ 55%.) |
| As noted patients treated with implant alone, must have ideal anatomy
(small gland, not TUTP defect) and early cancer that is likely confined to the gland (not
outside the capsule) The eligibility criteria from the current
RTOG trial (RTOG 98-05) is noted:
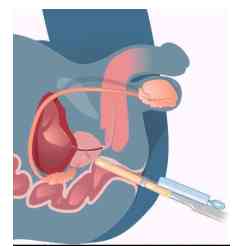
PHASE II TRIAL OF TRANSRECTAL
ULTRASOUND GUIDED PERMANENT RADIOACTIVE IMPLANTATION OF THE PROSTATE FOR DEFINITIVE
MANAGEMENT OF LOCALIZED ADENOCARCINOMA OF THE PROSTATE Patients will receive I-125
permanent implantation of the prostate, 146 Gy (TG 43) |
![]()
{kind=link}