|
|
|
|
|
|
|
|
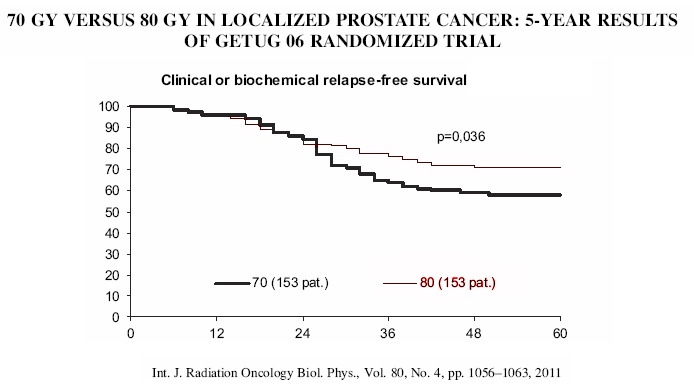
In the past, when using external beam radiation, the whole pelvis was treated to a dose of approximately 5000cGy (for the purpose of hitting the lymph nodes and adjacent areas where there may be early spread) and then an additional 1600 to 2000cGy was given to a small field (boost field) designed to hit only the prostate with a small area around it (often to include the seminal vesicles). As noted below the recommended dose is now up to 7500 - 8000cGy (go here). See the IMRT section here |

{kind=link}
{kind=link}