 |
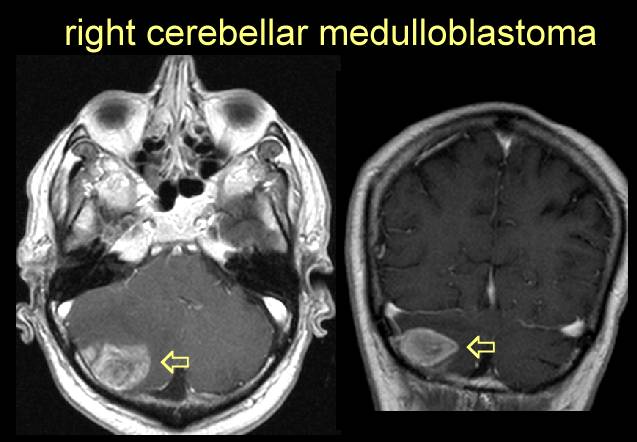
Medulloblastoma (see review, review, review, review, review, review) see stage, technique, technique, pictures, pictures
|
|
|
Medulloblastoma (see review, review, review, review, review, review) see stage, technique, technique, pictures, pictures
|
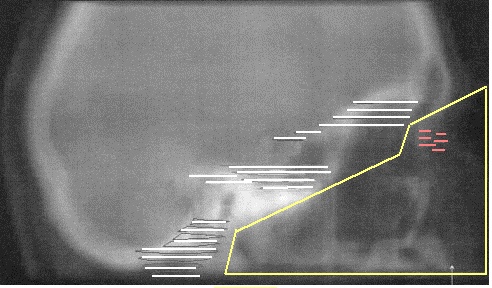
Impact of radiation technique upon the outcome of treatment for medulloblastoma.Halperin EC. IJROBP 1996;36:233 Duke University Medical Center Craniospinal irradiation (CSI) is an essential component of the therapy of medulloblastoma. Because medulloblastoma disseminates via the cerebrospinal fluid (CSF), CSI technique involves the irradiation of all CSF-bearing areas which are at risk for tumor seeding. Underdosing with radiation because of inadequacies in CSI technique will produce dose "cold spots" which have the potential of serving as a nidus for tumor recurrence. A simple mathematic model of subclinical disease in medulloblastoma based on the available data concerning the radiosensitivity of medulloblastoma cell lines as well as the known clinical dose-response relationships support the hypothesis that for most cases of medulloblastoma, the radiotherapist is working in a range of doses arrayed on the steep portion of the tumor control probability curve. Underdosing of CSF-bearing areas because of technical problems at the junction of the cranial and spinal fields of irradiation, placement of shielding blocks in the cribiform plate-subfrontal region, and/or anatomic errors in the design of the caudal end of the CSI fields may lead to significant risks of tumor relapse. One may debate the necessity of a posterior fossa boost encompassing the entire anatomic posterior fossa rather than the primary tumor volume with a margin. This review critically evaluates the potential impact of CSI technique upon the outcome of treatment for medulloblastoma, and suggests future areas of inquiry. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}