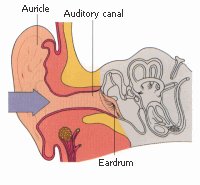
External Auditory Canal Cancer
Most patients present with symptomatic lesions of the external canal. Pruritus and pain
are common. Swelling behind the ear, decreased hearing, and facial paralysis are seen in
advanced cases. Spread of the tumor into the lymphatic areas is more common than to other
areas
of the ear. Tumors arising in the cartilaginous portion of the canal invade the
cartilaginous walls and spread into the bony canal areas. However, those arising in the
bony canal have a more effective barrier (preventing spread) and therefore progress
predominantly along the main axis of the canal, eventually invading the middle ear or the
cartilaginous part of the canal. Distant metastases are rarely seen with these
tumors.About 85% of the tumors involving the auditory canal, middle ear, and mastoid area
are squamous cell carcinomas. Infrequently, basal cell carcinomas, adenocarcinomas,
adenoid cystic carcinomas, and melanomas are seen.
Radical surgery and postoperative
radiation therapy are the accepted methods of treatment for more advanced lesions of the
external auditory canal and lesions in the middle ear and mastoid. Except in tumors that
are detected early, neither modality is considered optimal, and a combination of the two
produces the best results.Lesions of the outer part of the auditory canal require local
excision with at least a 1-cm margin between the lesion and the tympanic membrane if there
is no radiographic evidence of invasion of the mastoid. Surgery for tumors of the auditory
canal is performed through a U-shaped incision with elevation of the flap from below. A
split-thickness skin graft is usually required to cover the deficit along the auditory
canal.
When the tumor involves the bony auditory canal and impinges on the tympanic membrane but
does not involve the middle ear or the mastoid, a partial temporal bone resection may be
necessary; in this procedure the auditory canal, tympanic membrane, malleus, and incus are
removed
along with the temporomandibular joint, and the defect is grafted with a split-thickness
skin graft. Large lesions of the external auditory canal are treated with irradiation
alone or combined with surgery; the portals should encompass the entire ear and temporal
bone with an adequate margin (3cm). The volume treated should include the ipsilateral
preauricular, postauricular, and subdigastric lymph nodes. Treating lymphatics
beyond the jugulodigastric area is usually not necessary.
Extremely advanced tumors that are unresectable should be treated with high-energy
ipsilateral electron-beam therapy (16 to 20 MeV) alone or mixed with photons (4 to 6 MV)
or with wedge pair (superior inferiorly angled beams) techniques using low-energy photons.
Doses of 60 to 70 Gy over 6 to 7 weeks are required. |
{kind=link}