|
|
|
|
|
|
Ductal
Carcinoma In Situ
(DCIS)
|
|
|
|
|
|
Ductal
Carcinoma In Situ
(DCIS)
|
|
 |
Generally after lumpectomy the woman will
receive radiation, but if the cancer is estrogen + she may be a candidate
for Tamoxifen and if the cancer is HER2 + she may even be a candidate for
Herceptin (go here and
here). For recent data on the risk of relapse by
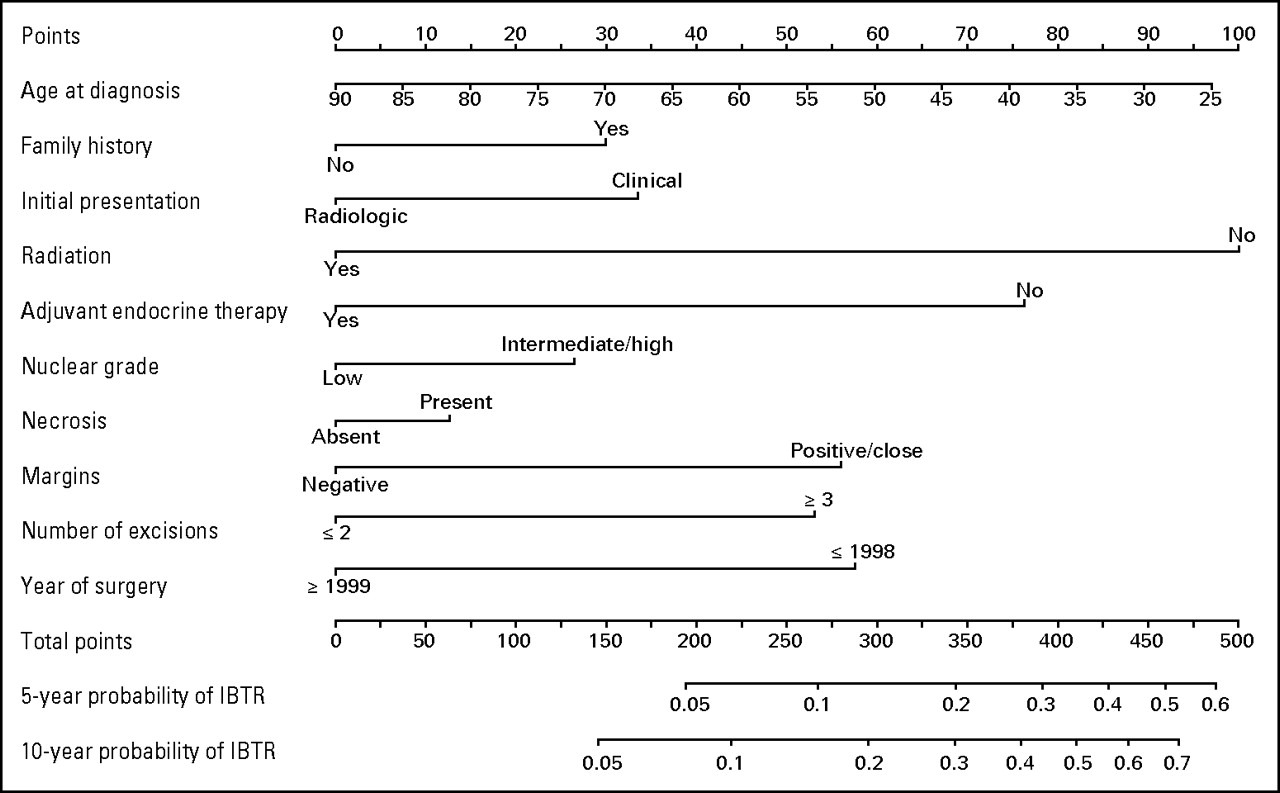
treatment go here and for nomogram go
here/ (See recent New England Journal Review.) Another recent consensus report was published on treatment of DCIS (Cancer 2000;88:946) They noted that lumpectomy alone may be considered if the tumor is less than 2-3 cm, with margins 10mm or greater, with low or intermediate grade. Even in the lumpectomy radiation group they considered a margin of 10mm optimal for best local control. Another recent review noted that close margins (2 -3mm or less) had no worse a local relapse rate as those with negative margins, see other recent trial on margins suggesting that 2mm margins are adequate. |
| Note that the current standard of care is
generally lumpectomy, no node dissection then radiation. Based on the new data from NSABP B-24 it may be useful to add Tamoxifen
as well. The B-24 study enrolled 1804 women diagnosed with DCIS (or DCIS plus
Lobular Carcinoma In Situ (LCIS)) who had a lumpectomy and radiation therapy between
1990-1994. Half of the women were prescribed tamoxifen, 20 mg daily for five years, and
half placebo. Researchers found that adding tamoxifen significantly reduced
the incidence of all invasive and non invasive breast cancers at any site by 37%,
from 13.4 percent in the placebo group (130 cases) to 8.2% in the tamoxifen-treated group
(84 cases) In analyzing all invasive breast cancers, tamoxifen
reduced the incidence over five years by 43%, from 7.2% in the placebo group (70 cases) to
4.1% in the tamoxifen-treated group (41 cases) (p=.004). Also note that the standard of care is to not perform lymph node dissection (since the risk of lymph node spread if there is no microinvasion is thought to be close to 0%.) Recent studies using sentinel node biopsies and special staining of the nodes have found the risk of occult node spread may be as high as 8% as noted: " A significant expansion of the precision of sentinel lymph node diagnostics has occurred with the application of molecular and immunohistochemical markers to detect occult metastases. More intensive examination of these nodes occurs and more accurate staging results in DCIS patients with occult micrometastases to the regional lymphatic basin staged with greater precision. Our studies have shown that the seeming lack of microinvasion in the primary lesion does not prevent the presence of nodal disease. Data from consecutive prospective series of 1,147 breast cancer patients who underwent lymphatic mapping are noted and all patients with a preoperative diagnosis of DCIS, regardless of size or pathologic staging, were evaluated with sentinel lymph node biopsy. Positive sentinel lymph nodes were found in 8.6% of the T0 or presumed pure DCIS patients" |


{kind=link}
{kind=link}
{kind=link}