Ductal Carcinoma
in Situ of the Breast
Harold J. Burstein, NEJM 2004;350:1430
Ductal carcinoma in situ of the breast (also called intraductal carcinoma) consists of the clonal proliferation of cells that appear malignant and that accumulate within the lumens of the mammary duct. There is no evidence of invasion beyond the epithelial basement membrane into the adjacent breast stroma. This lesion, which is a precursor to invasive ductal carcinoma, is frequently diagnosed on screening mammography. In the past 20 years, concomitant with the wide use of screening mammography, the incidence of ductal carcinoma in situ has risen dramatically, and data from large cohort studies and randomized trials have emerged to guide treatment. Furthermore, advances in molecular biology are providing important insights into the relationship between ductal carcinoma in situ and invasive breast cancer. This review summarizes progress in the understanding and therapy of ductal carcinoma in situ.
Biologic Characteristics
Ductal carcinoma in situ lies along a spectrum of preinvasive lesions originating within normal breast tissue, with histologic progression from atypical hyperplasia to invasive breast cancer (Figure 1) Although the initiating steps and precise pathways of breast tumorigenesis remain poorly defined, it appears that nearly all invasive breast cancers arise from in situ carcinomas. The presence of shared chromosomal changes in both ductal carcinoma in situ and synchronous, adjacent invasive cancers demonstrates their clonal, evolutionary relationship.
|
Multiple clinicopathological and biologic features distinguish ductal carcinoma
in situ from both normal breast tissue and other benign proliferative breast
lesions. Chromosomal imbalances occur, with gain
or loss at multiple loci, as hyperplastic lesions progress through ductal
carcinoma in situ to invasive breast cancer. For instance, loss of heterozygosity is noted in more than 70 percent of
high-grade ductal carcinomas in situ, as compared with 35 to 40 percent of
cases of atypical hyperplasia and 0 percent in specimens of normal breast
tissue.Molecular markers associated with breast tumorigenesis have been
identified. The estrogen receptor — normally
expressed by luminal breast epithelial cells — is expressed by over 70
percent of ductal carcinoma in situ lesions. The HER2/neu proto-oncogene
is overexpressed in roughly half of all ductal carcinoma in situ lesions
but not in atypical hyperplasia.The p53 tumor-suppressor gene is mutated
in approximately 25 percent of all ductal carcinoma in situ lesions, but is
rarely mutated in normal or benign proliferative breast tissue.The frequency
with which these molecular markers are expressed in ductal carcinoma in situ
generally mirrors their expression in invasive breast cancers.
Genomicand proteomic approaches have identified numerous differences in patterns of gene and protein expression between normal or hyperplastic breast tissue and ductal carcinomas in situ. Factors known to be related to cell growth and differentiation, cytoskeletal function, intracellular transport of cell membranes, and the function of the surrounding microenvironment have been examined. The most dramatic changes in patterns of gene expression during breast tumorigenesis appear during the transition from normal tissue to ductal carcinoma in situ. In contrast, the gene-expression profile of ductal carcinoma in situ is quite similar to that of invasive breast cancer.Genes that are uniquely associated with invasive tumors have not been identified, which suggests that many of the hallmark cellular events specific to the transformation process in breast cancer arise during or before the development of ductal carcinoma in situ.
Ductal carcinoma in situ is biologically heterogeneous, with variable
pathological, molecular, and clinical features. For instance, the
gene-expression profile of high-grade ductal carcinoma in situ differs from
that of low-grade lesions and exhibits a greater overall genetic change from
normal breast tissue. There is good, if incomplete, concordance between
synchronous ductal carcinoma in situ and invasive tumors with respect to the
tumor grade, estrogen-receptor status, HER2/neu status, and p53
status, although these markers have a heterogeneous distribution of expression.
More than 90 percent of low-grade ductal carcinoma in
situ lesions are positive for estrogen receptors, and less than 20 percent
exhibit overexpression of HER2/neu or p53 mutations. In contrast,
overexpression of HER2/neu or p53 mutations arise in two thirds
of high-grade ductal carcinoma in situ lesions, whereas only one quarter
express estrogen receptors.
Data suggest that ductal carcinoma in situ represents a stage in the development of breast cancer in which most of the molecular changes that characterize invasive breast cancer are already present, though the lesion has not assumed a fully malignant phenotype. A final set of events, which probably include gain of function by malignant cells and loss of function and integrity by surrounding normal tissues, is associated with the transition from a preinvasive ductal carcinoma in situ lesion to invasive cancer. Most, if not all, clinically relevant features of breast cancer, such as hormone-receptor status, the level of oncogene expression, and histologic grade, are probably determined by the time ductal carcinoma in situ has evolved Thus, the variable clinical characteristics of invasive breast cancer may be explained by the heterogeneous nature of the preceding ductal carcinoma in situ lesions.
Clinical and Pathological Features
With the introduction of widespread screening mammography, the incidence of ductal carcinoma in situ has increased by a factor of 10 in the past two decades, from 4800 cases in 1983 to more than 50,000 cases now diagnosed annually in the United States.Ductal carcinoma in situ accounts for nearly 20 percent of all breast cancers detected by screening (1 case of ductal carcinoma in situ detected per 1300 screening mammograms) in North America.
Older age, benign breast disease, a family history of breast cancer, and reproductive factors such as nulliparity or an older age at the time of the first full-term pregnancy are all associated with an increased risk of both invasive breast cancer and ductal carcinoma in situ. Population-based models that use family history and demographic data predict that 5 percent of women with ductal carcinoma in situ carry a mutation in the BRCA1 or BRCA2 hereditary cancer gene. Postmenopausal hormone-replacement therapy may increase the risk of ductal carcinoma in situ. Like invasive breast cancer, ductal carcinoma in situ overwhelmingly affects women; it is rare among men.
Before the use of screening mammography became widespread, ductal carcinoma in situ was diagnosed after the finding of a palpable breast mass or thickening or nipple discharge or after the diagnosis of Paget's disease of the nipple. In contrast, currently, nearly 90 percent of ductal carcinomas in situ are diagnosed while they are clinically occult because of mammographic detection of microcalcifications (in 76 percent of cases), soft-tissue densities (11 percent), or both (13 percent). Calcification patterns on mammography are only moderately correlated with pathological types of ductal carcinoma in situ.
Microcalcifications in the breast are frequently evaluated by stereotactic core needle biopsy; they can be benign or malignant. Patients with atypical ductal hyperplasia that has been identified on core needle biopsy should undergo wider, surgical biopsy because 10 to 50 percent of such lesions may include ductal carcinoma in situ or invasive cancer on subsequent excision.Similarly, patients with ductal carcinoma in situ that is diagnosed on core needle biopsy require surgical excision to remove the ductal carcinoma in situ and rule out associated invasive carcinoma, which is found on excision in approximately 10 to 15 percent of cases — a likelihood that increases with the grade of ductal carcinoma in situ.
The crucial task on pathological assessment is to distinguish ductal carcinoma in situ from invasive cancer. The pathological classification of ductal carcinoma in situ is based on the nuclear grade of the tumor cells (low, intermediate, or high), the architectural pattern of tumor growth (solid, papillary, micropapillary, or cribriform), and the presence or absence of comedonecrosis. Classification remains a challenge owing to differing pathological criteria, interobserver variability, and the heterogeneous nature of tumor growth. High-grade lesions and lesions associated with comedonecrosis are associated with the greatest risk of recurrence after breast-conserving surgery.
|
| Trial | Local Relapse | Local Relapse | Local Relapse | Opposite Breast |
| Lumpectomy Only | Lump + XRT | Lump+XRT+Tamoxifen | ||
| NABP B17 | 16% (5y) | 7% (5y) | 6.6% | |
| 27% (12y) | 12% (12y) | |||
| EORTC | 16% (4y) | 9% (4y) | 3% | |
| NSABP B24 | 9% (5y) | 6% (5y) | 2% (Tam) 5% (no Tam) | |
| 11% (7y) | 8% (7y) | |||
| UKCCCR | 14% (5y) | `6% (5y) | 2% |
Discontinuous growth within the ductal system of the breast and the irregular
nature of associated calcifications make the extent of ductal carcinoma in situ
difficult to determine. Ductal carcinoma in situ originates in a single
glandular structure but may spread within the breast through the ductal
system.Two thirds of patients with low-to-intermediate-grade ductal carcinoma
in situ have multifocal disease, characterized by discontinuous intraductal
growth, with gaps of up to 1 cm between tumor foci. In contrast, high-grade
lesions tend to be continuous, with most having no gaps greater than 5 mm.
Because of the discontinuous spread of ductal carcinoma in situ through the
ductal system, the use of standard mammographic views may underestimate the
extent of the lesion, especially in the case of low- and intermediate-grade
tumors. Thus, magnification views are warranted. True multicentric ductal
carcinoma in situ, originating in two discrete ductal systems, is uncommon.
Ductal carcinoma in situ may be associated with an occult microinvasive tumor (one that does not exceed 0.1 cm in diameter). Such cases are classified as microinvasive breast cancer and are generally treated according to the guidelines for invasive disease. Occult microinvasive tumors are most common in patients with ductal carcinoma in situ lesions that are greater than 2.5 cm in diameter,those presenting with palpable masses or nipple discharge, and those with high-grade ductal carcinoma in situ or comedonecrosis.
The natural history of untreated low-grade ductal carcinoma in situ has been defined in long-term, follow-up studies of women who underwent diagnostic biopsy alone in the era before widespread screening mammography. After 10 years of follow-up, 14 to 60 percent of the women had received a diagnosis of invasive cancer in the affected breast. Such risk is widely thought to justify present treatment approaches to ductal carcinoma in situ. The natural history of untreated high-grade ductal carcinoma in situ or ductal carcinoma in situ detected clinically is not well characterized, since in most cases, the tumor has been fully excised surgically.
Treatment
The goal in treating ductal carcinoma in situ is prevention of local recurrence — in particular, invasive breast cancer. The options for surgical treatment include simple mastectomy or breast-conserving surgery (often called lumpectomy, though in most cases, there is no lump), with only the affected areas of the breast excised. Mastectomy and breast-conserving surgery as treatments for ductal carcinoma in situ have not been compared in prospective, randomized trials. Data from some surgical trials and large treatment registries suggest that the rates of local or regional recurrence are significantly lower after mastectomy than after breast-conserving surgery, but there have been no significant differences in overall survival. Metastatic breast cancer can follow the recurrence of an invasive tumor or the development of cancer in the contralateral breast. However, death related to breast cancer within 10 years after the diagnosis of ductal carcinoma in situ occurs in only 1 to 2 percent of all patients, irrespective of whether mastectomy or breast-conserving surgery was performed.
Historically, ductal carcinoma in situ was treated with mastectomy. Simple mastectomy is highly effective for ductal carcinoma in situ — curing at least 98 percent of lesions — and is a potential treatment option for all patients. Breast cancer recurs in 1 to 2 percent of patients with ductal carcinoma in situ who have undergone mastectomy, owing to the presence of occult invasive disease at the time of diagnosis, recurrence within residual breast tissue, or contralateral breast cancer. Women with ductal carcinoma in situ in one breast are at risk for a second tumor (either invasive or in situ) in the contralateral breast; the rate at which such tumors develop is similar to that among women with primary invasive breast cancer — approximately 0.5 to 1 percent per year.
At the present time, most women in the United States are treated with breast-conserving surgical excision. This pattern reflects the detection of smaller, clinically occult ductal carcinoma in situ lesions with the use of mammography and the shift in treatment toward breast-conserving surgery for invasive breast cancer, after the demonstration that modified radical mastectomy and breast-conserving surgery are associated with equivalent survival rates.It seems paradoxical to offer more extensive surgery for preinvasive cancer than for invasive cancer. Early studies of the treatment of ductal carcinoma in situ with excision alone as compared with excision and radiotherapy showed acceptably low recurrence rates that justified further exploration of breast conservation.
After breast-conserving surgery for ductal carcinoma in situ, women are at risk for recurrence within the breast. Half the recurrences in the ipsilateral breast are invasive tumors, and half are ductal carcinoma in situ. Most recurrences are at or near the original site of the tumor, with pathological features that are similar to those of the index lesion, including shared histologic features such as the grade and expression of estrogen receptor and HER2, as well as clonal genetic features. Thus, although true second cancers may occur, most recurrences in the ipsilateral breast arise from residual microscopical disease at or near the original site of the tumor.
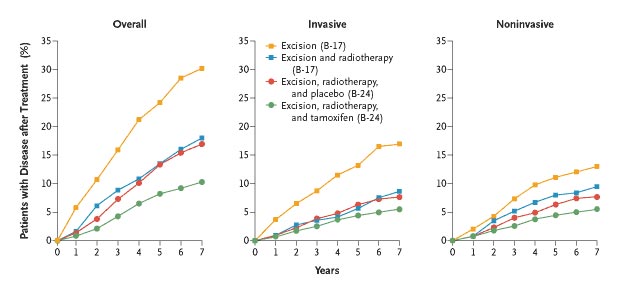
Principles for managing ductal carcinoma in situ in women who have undergone breast-conserving surgery have been defined on the basis of large, prospective, randomized clinical trials. Three randomized trials directly compared excision alone with excision and radiotherapy for fully excised ductal carcinoma in situ among patients with negative margins, defined as the absence of tumor at the inked surgical surface.Most patients in these studies had small areas of ductal carcinoma in situ (less than 2 cm in diameter), detected with mammography. Radiotherapy consistently reduces the risk of recurrence in the ipsilateral breast by 40 to 60 percent. At five years of follow-up, excision alone is associated with approximately a 16 percent risk of recurrence in the ipsilateral breast; radiotherapy reduces this risk to approximately 8 percent. These relative benefits persist for at least 12 years, though the absolute risk of recurrence continues to increase over time. In two large international-registry studies of the treatment of ductal carcinoma in situ, the rates of local recurrence were 16 and 19 percent at 15 years among women who were treated with breast-conserving surgery and radiation — results that are generally consistent with those of randomized trials.
|
The selective estrogen-receptor modulator tamoxifen has also been studied as
adjuvant therapy in women with ductal carcinoma in situ who have undergone
excision and radiation treatment. In the B-24 trial of the National Surgical
Adjuvant Breast and Bowel Project (NSABP), tamoxifen reduced the likelihood of
recurrence in the ipsilateral breast at five years from 9 to 6 percent, an
absolute risk reduction of 3 percent, and reduced the risk of a tumor in the
contralateral breast . In a related study with a two-by-two factorial design in
which patients were randomly assigned to radiation or no radiation and
to tamoxifen or no tamoxifen, the women who received both radiotherapy and
tamoxifen had the lowest rate of recurrence in the breast; however, the
additional benefits of tamoxifen were small and did not reach statistical
significance. Tamoxifen may be especially valuable in preventing ipsilateral
tumor recurrence among patients also receiving radiotherapy, as has been
demonstrated in the treatment of small, invasive breast cancers.There
is no role for chemotherapy in the treatment of ductal carcinoma in situ.
In a preliminary retrospective analysis, estrogen-receptor expression was a marker of a benefit of tamoxifen in patients with ductal carcinoma in situ. Tamoxifen reduced the risk of recurrence by 60 percent in patients with estrogen-receptor–positive ductal carcinoma in situ, whereas the risk reduction for estrogen-receptor–negative lesions was not statistically significant. Thus, as with invasive breast cancer, the role of tamoxifen in the treatment of ductal carcinoma in situ may be limited to tumors that are estrogen-receptor positive, but this awaits confirmation. the risk of recurrence in the ipsilateral breast or a tumor in the contralateral breast among women treated with excision alone, excision and radiation, or excision, radiation, and tamoxifen in the NSABP randomized trials.
The predictors of recurrent tumor after breast-conserving surgery for ductal carcinoma in situ have been extensively studied. Close (less than 1 mm) or positive surgical margins and high-grade or comedonecrotic lesions are associated with an increased risk of local recurrence. Subgroup analyses from randomized trials have demonstrated that the absolute benefits of radiotherapy are greater in women at increased risk for tumor recurrence, such as women with involved surgical margins (identified on retrospective pathological review), younger women, and those with tumors that have high-grade or comedonecrotic features. However, radiotherapy still lowers the incidence of recurrence among all such subgroups, regardless of the base-line risk.
Younger age (usually defined as less than 40 or less than 45 years) is a significant predictor of recurrence after breast-conserving surgery. Younger age is also associated with other adverse clinical factors, including a higher tumor grade or necrosis, clinical (as opposed to mammographic) findings on presentation, and more extensive disease. Some data suggest that younger women are treated with less extensive resection of ductal carcinoma in situ at the time of lumpectomy. However, none of these factors in themselves make younger patients ineligible for breast-conserving therapy.
Ipsilateral tumor recurrences in patients with ductal carcinoma in situ are usually detected on surveillance mammography, although one quarter may be detected on the basis of changes on physical examination of the breast or chest wall.For this reason, patients should be scheduled for a base-line mammogram 6 to 12 months after initial therapy and at least annually thereafter. Distant breast-cancer metastases in the absence of regional recurrence are unusual. Local recurrences after breast-conserving surgery and radiotherapy are generally treated with mastectomy. Selected patients with local recurrences who have not previously received radiotherapy may be candidates for local excision and radiotherapy. The clinical outcome of ipsilateral tumor recurrence is governed by the nature of the recurrence. Patients with recurrent ductal carcinoma in situ have an excellent prognosis, with less than a 1 percent risk of further recurrence after salvage mastectomy. Patients with invasive recurrence after breast-conserving surgery for ductal carcinoma in situ have a prognosis similar to those with early-stage breast cancer, with a 15 to 20 percent risk of metastatic recurrence at eight years.
Clinical Management
Patients are first assessed to determine whether they are candidates for
breast-conserving surgery. Women with multicentric ductal carcinoma in situ, as
defined by the presence of two or more tumors in separate quadrants of the
breast, and those with extensive or diffuse ductal carcinoma in situ or
suspicious-appearing microcalcifications throughout the breast are candidates
for mastectomy, as are women in whom negative margins or acceptable cosmesis
cannot be achieved with the use of breast-conserving surgery. Similarly, women
who are not candidates for radiotherapy because they have a collagen vascular
disease such as scleroderma or active systemic lupus erythematosus, have
previously undergone radiotherapy, or are pregnant should be offered
mastectomy. Some women may prefer mastectomy to breast conservation in order to
minimize the chance of ipsilateral recurrence or for other reasons. At present,
there is no established role for the use of magnetic resonance imaging in
screening patients for ductal carcinoma in situ or in determining whether
breast-conserving surgery is an option.
Patients deemed to be appropriate candidates for breast conservation require
complete surgical excision of the affected area. Careful orientation marking of
the surgical specimen may facilitate subsequent reexcision, if necessary. The
extent of ductal carcinoma in situ in the breast90
and the existing margin determine the likelihood of identifying residual
disease on reexcision. Nearly half of patients with margins that are less than
1 mm have residual ductal carcinoma in situ on reexcision. However, the optimal margin width for the management of
ductal carcinoma in situ is not known. At a minimum, there should be no tumor
at the margin. Margins with a width of 1 mm or more are associated with
a reduced risk of recurrence, a reasonable treatment goal.
Neither dissection of axillary lymph nodes nor mapping of sentinel lymph nodes is routinely warranted in patients with ductal carcinoma in situ, owing to the very low incidence of axillary metastases. Three to 13 percent of patients with ductal carcinoma in situ, and a slightly greater percentage with ductal carcinoma in situ characterized by microinvasion, have isolated tumor cells in sentinel axillary lymph nodes. The prognostic significance of these cells is not clear. Clinical experience suggests that patients have a much better outcome than would be predicted by such rates of nodal metastases, and the vast majority of instances represent micrometastases of unclear metastatic potential. However, sentinel-lymph-node mapping may be used in selected patients with a higher likelihood of occult invasive cancer — those with extensive, high-grade ductal carcinoma in situ or palpable masses — and those undergoing mastectomy, since sentinel-node mapping cannot be performed afterward if invasive tumor is identified.
After breast-conserving surgery, radiotherapy is administered in tangential fields to the whole breast. The standard dose, 44 to 50 Gy delivered in fractions of 180 to 200 cGy on a daily basis, results in control of the tumor, and in most cases, the cosmetic outcome is rated as good to excellent. On the basis of extrapolation from data on the treatment of invasive breast cancer, a radiation boost to the tumor bed may be added to whole-breast treatment, particularly for women with close surgical margins, although the benefits of such therapy for the management of ductal carcinoma in situ are not well characterized. Partial-breast irradiation has not been studied in patients with ductal carcinoma in situ. There is no proven role for postmastectomy or nodal irradiation in the treatment of ductal carcinoma in situ.
Methods of identifying patients with ductal carcinoma in situ who may not require radiotherapy after excision of the tumor are being investigated. A retrospective analysis has suggested that patients with low-grade, small tumorsor lesions with margins greater than 10 mm have a very favorable prognosis, which may not be improved by radiotherapy. To date, this finding has not been confirmed in prospective studies of wide excision alone as therapy for ductal carcinoma in situ. In a study of women who had small areas of low- or intermediate-grade ductal carcinoma in situ, with negative reexcisions or margins of at least 1 cm, the recurrence rate was 12 percent five years after excision alone — a substantially higher rate than that predicted on the basis of retrospective analyses.Thus, it is not yet possible to identify prospectively women who are at sufficiently low risk that radiotherapy may not be of some clinical advantage in preventing recurrences. After discussing the various options, patients may elect not to receive radiation treatment, but they must understand and accept the increased risk of recurrence that this choice probably entails.
Surveys of patients have shown that women with ductal carcinoma in situ have considerable deficits in their knowledge of the disease and that their levels of psychological distress and fear of recurrent disease and death are similar to those among women with invasive breast cancer. Clinicians can address their patients' misconceptions by providing accurate information and counseling.
Because ductal carcinoma in situ is a precursor to invasive breast cancer and shares many biologic features of invasive disease, it is increasingly recognized as a target for preventive measures. In the largest trials of the prevention of primary breast cancer among women at high risk for breast cancer by virtue of age, family history, or prior benign breast disease, tamoxifen reduced the risk of ductal carcinoma in situ by 50 to 70 percent.
In summary, ductal carcinoma in situ is a preinvasive breast tumor commonly detected in women undergoing screening mammography. Ductal carcinoma in situ is heterogeneous, with a spectrum of biologic and clinical features affecting the likelihood of transformation to invasive breast cancer and recurrence within the affected breast. The goal of treatment is to reduce the risk of recurrent disease in the breast, particularly invasive cancer. A variety of treatment options are available to patients, but there are no data showing that any one strategy provides superior survival. The treatment options vary with respect to the risk of a recurrence in the ipsilateral breast and side effects. Treatment choices are complicated by the varied clinical behavior of ductal carcinoma in situ. Patients and clinicians can use available data on likely benefits and potential side effects of therapy to make well-informed treatment decisions.
{kind=link}
{kind=link}