|
|
|
|
|
|
Treating Glioblastoma

|
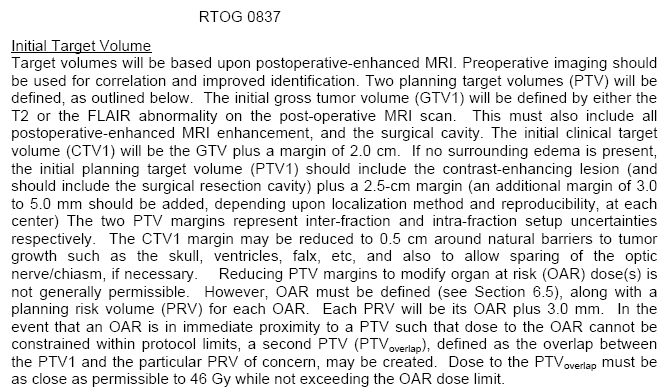
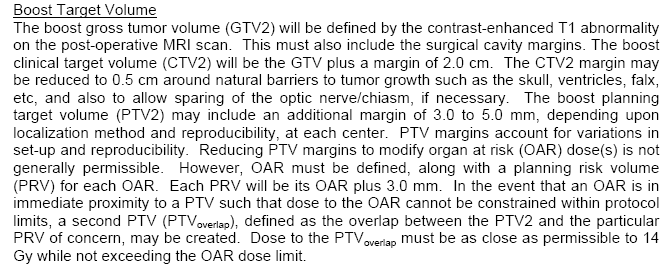
.Patients generally have surgery and as much tumor as can be safely resected is removed. (See recent discussion of the limits of brain surgery here.) This is followed by radiation (external beam to 60Gy) with or without chemotherapy (e.g. Temodar). See the current NCCN information here. New drugs are finally showing promise (go here) and there may be benefit from high dose Temodar (go here). A recent update on treatment is here. The tumor invariably comes back. Because of this discouraging outcome, there are dozens of research trials going on, trying to improve the results with this cancer. (The recent RTOG trial combined weekly Taxol with XRT (60Gy) with no improvement in survival, median of 9.7 mos Langer. IJROBP 2001;51:113.) A recent trial combined radiation with CCNU and Temodar with good results (go here). See the section on chemotherapy here Typical dose schemes and port sizes from the RTOG are here are target advice from RTOG 0825 for PTV1 here and PTV2 here and dose limits here. Targets from RTOG 0837 are here and here. Other target information here. To encompass infiltrating tumor cells, the RT dose (typically 60 Gy) is usually delivered to the tumor plus a margin of radiographically apparently normal tissue. If the tumor is defined based upon contrast enhancement, a margin of 2.0 to 3.0 cm is often used, while if the RT field is defined by T2-weighted MRI abnormality, a 1.0 to 2.0 cm margin is used. |


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}