|
|
|
|
|
|
|
|
|
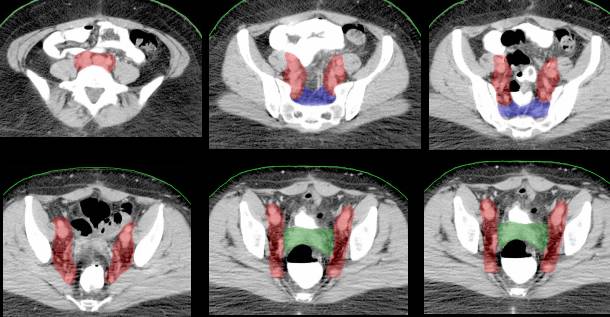
IMRT field (blue) surrounding the cervix cancer (red) and the involved lymph nodes (green) |

We
participate with the GOG (Gynecologic Oncology Group) which
conducts national (international) research trials concerning the
treatment of gynecologic cancer.
For more information go here, and for typical radiation
fields used in the GOG protocols. More
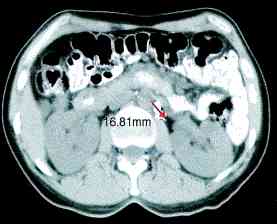
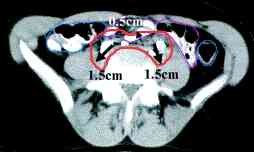
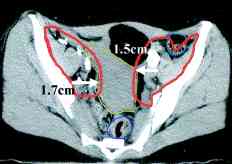
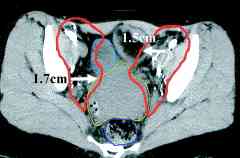
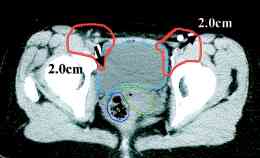
cervix ports, the node positions on CT scans (IJROBP
2002;54:1147) (A) Furthest
distance from lymph node to vessel wall. (B)
Para-aortic lymph node CTV. (C)
Common iliac lymph node CTV. (D)
External iliac CTV, including lateral group. (E) External
iliac CTV, including medial (obturator) group. (F)
Inguinal lymph node CTV. CTV depicted by thick orange line.
Small bowel demarcated by thin magenta, large bowel by thin
blue, rectum by thin dark purple, bladder by thin turquoise, and
uterus by thin yellow-green line. RTOG atlas
here and here
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
AP
Pelvis Field (MRI appearance)
Lateral Pelvic Field (MRI appearance)
Para-Aortic
Node Field
Inguinal/Vulva Field
Whole Abdominal
Field
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}