| Trigeminal neuralgia (TN), or tic
douloureux, is a chronic, episodic facial pain syndrome, with onset most commonly in the
sixth or seventh decades of life. It affects about 4.3 per 100,000 people annually, and is
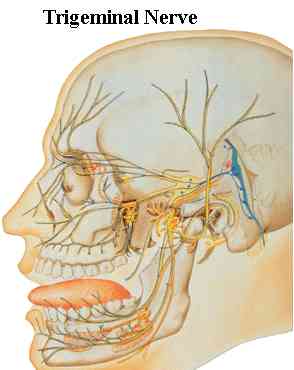
often debilitating. It can involve one or more divisions of the trigeminal nerve, and is
characterized by five classical features being: paroxysmal, provokable, unilateral,
confined to the trigeminal nerve domains, and unassociated with gross trigeminal motor or
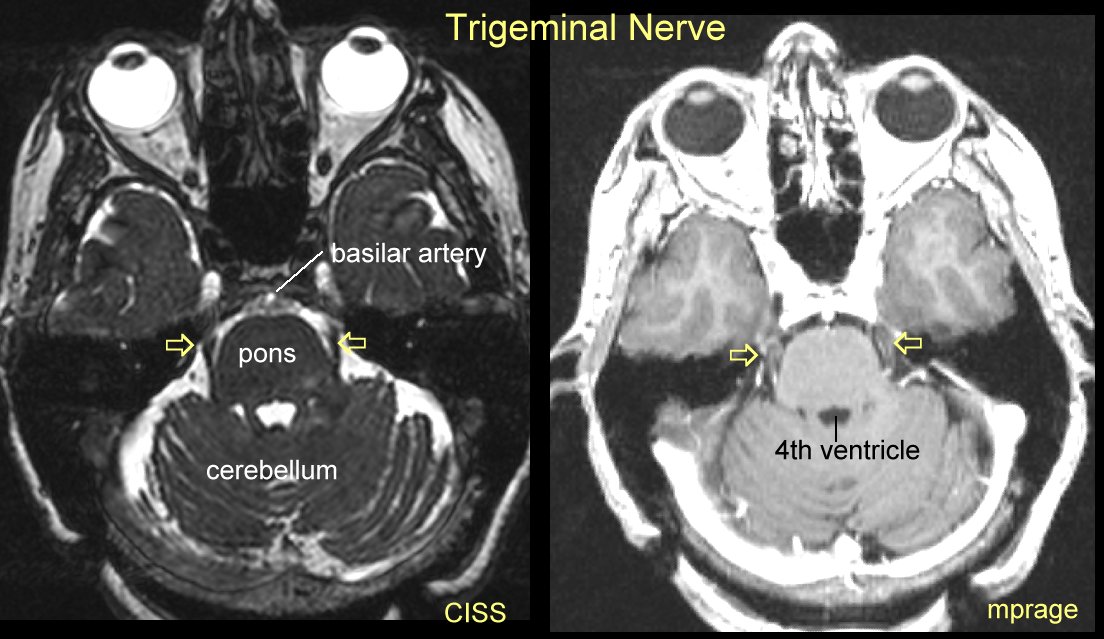
sensory loss. The etiology of TN has been
ascribed to a blood vessel compressing the trigeminal root at its junction with the pons,
thus altering axonal transmission. However, only rarely is an anatomic abnormality
demonstrable on imaging studies, either in the peripheral or central pathways of the
affected trigeminal nerve.
The initial management of tic pain consists of
medical therapy, such as carbamazepine, phenytoin, gabapentin, or baclofen. When medical
therapy is ineffective or causes intolerable side effects, surgical intervention becomes
necessary. In general patients
should start with medication first (go
here) before considering
radiosurgery. The most commonly used medications include Tegretol,
Trileptal, Lamictal, Lyrica and Neurontin (go
here).
Surgical options include decompression of the affected nerve (retromastoid
craniectomy with microvascular decompression of the trigeminal nerve) and various
percutaneous rhizotomies of the trigeminal nerve using heat, mechanical compression,
radiation, or osmotic injury to interrupt the pain transmission. Microvascular
decompression entails higher operative risks, and trigeminal rhizotomy procedures are
associated with deafferentation of the face. Although microvascular decompression is a
potentially curative procedure for eligible healthy patients, many patients with tic
douloureux are elderly or have medical contraindications to invasive surgery.
Approximately 30% of patients who undergo initial microvascular decompression eventually
have a relapse. Retrogasserian radiosurgical rhizotomy is a relatively noninvasive and
safe procedure that is suitable for patients with and without a history of prior surgery |





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}