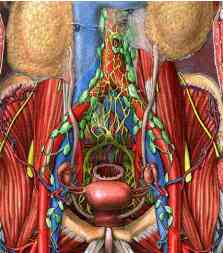
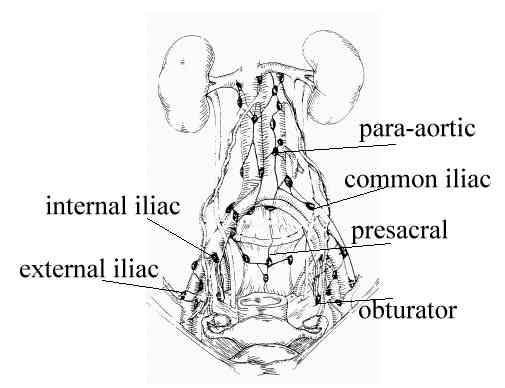
Potential therapeutic role of para-aortic
lymphadenectomy in node-positive endometrial cancer.
Mariani A, Webb MJ, Galli L, Podratz KC Gynecol Oncol 2000
Mar;76(3):348-56
Section of Gynecologic Surgery, Mayo Clinic and Mayo Foundation, Rochester, Minnesota
55905, USA.
The aim of this study was to assess the potential therapeutic role of para-aortic
lymphadenectomy (PAL) in high-risk patients with endometrial cancer. METHODS: We studied
two groups of patients with endometrial cancer who underwent operation at Mayo Clinic
(Rochester, MN) during the interval 1984 to 1993: (1) 137 patients at high risk for
para-aortic lymph node involvement (myometrial invasion >50%, palpable positive pelvic
nodes, or positive adnexae), excluding stage IV disease, and (2) 51 patients with positive
nodes (pelvic or para-aortic), excluding stage IV disease. By our definition, PAL required
removal of five or more para-aortic nodes. RESULTS: In both groups, no significant
difference existed between patients who had PAL (PAL+) and those who did not (PAL-) in
regard to clinical or pathologic variables, percentage irradiated, or surgical or
radiation complications. Among the 137 high-risk patients, the 5-year progression-free
survival was 62% and the 5-year overall survival was 71% for the PAL- group compared with
77 and 85%, respectively, for the PAL+ group (P = 0.12 and 0.06, respectively). For the 51 patients with positive nodes, the 5-year progression-free
survival and 5-year overall survival for the PAL- group were 36 and 42% compared with 76
and 77% for the PAL+ group (P = 0.02 and 0.05, respectively). Lymph node
recurrences were detected in 37% of the PAL- patients but in none of the PAL+ patients (P
= 0.01). Multivariate analysis suggested that submission to PAL was a cogent predictor of
progression-free survival (odds ratio = 0.25; P = 0.01) and overall survival (odds ratio =
0.23; P = 0.006). CONCLUSIONS: These results suggest a potential therapeutic role for
formal PAL in endometrial cancer. Copyright 2000
FIGO stage IIIC endometrial carcinoma with metastases confined to pelvic lymph nodes: analysis of treatment outcomes, prognostic
variables, and failure patterns following adjuvant radiation therapy.
Nelson G, Randall M, Sutton G, Moore D, Hurteau J, Look K Gynecol Oncol
1999 Nov;75(2):211-4
Department of Radiation Oncology, Indiana University Medical Center, Indianapolis, Indiana
46202, USA.
OBJECTIVES: This study was undertaken to evaluate the prognostic significance of isolated
positive pelvic lymph nodes on survival and to analyze other prognostic variables, overall
survival, and failure patterns in surgically staged endometrial carcinoma patients with
positive pelvic lymph nodes and negative para-aortic lymph nodes following radiation
therapy (RT). METHODS: Between January 1, 1987, and December 31, 1997, 782 women underwent
primary treatment for uterine cancer at Indiana University Medical Center. Through a
review of the medical records, we identified 58 patients with pathologic stage IIIA, 27
patients with pathologic stage IIIB, and 77 patients with pathologic stage IIIC
endometrial carcinoma. Patients with pathologically positive or unsampled para-aortic
lymph nodes and patients who received preoperative radiation therapy were excluded,
leaving a study group of 17 patients with nodal metastases confined to pelvic lymph nodes.
Thirteen patients received adjuvant pelvic RT using AP-PA or four-field technique. A
median dose of 5040 cGy was delivered. Four patients received whole abdominal irradiation
(WAI) delivering a median dose of 3000 cGy. Two patients received vaginal cuff boosts of
1000 and 3560 cGy to 0.5 cm from the vaginal surface mucosa via Cs-137 brachytherapy. Two
patients also received adjuvant chemotherapy (cis-platinum and doxorubicin) and/or
hormonal therapy (megestrol acetate). Disease-free and overall survivals were estimated
using the Kaplan-Meier method of statistical analysis and prognostic variables were
analyzed using the log-rank test. RESULTS: With a median follow-up of 51 months the actuarial 5-year disease-free survival was 81% and the actuarial 2-year
and 5-year overall survival rates were 81 and 72%, respectively. CONCLUSION:
Surgery followed by postoperative pelvic RT is a viable treatment option for
pathologically staged stage IIIC endometrial carcinoma with disease confined to the pelvic
lymph nodes. Failures in the para-aortic region suggest a possible role for extended-field
RT. Patients with positive peritoneal cytology in conjunction with nodal metastasis fared
poorly with pelvic RT. Studies evaluating the efficacy of WAI are ongoing. Finally,
substages within FIGO stage IIIC are recommended in an effort to better understand and
define treatment strategies which might be appropriate for these patients.
Endometrial cancer with para-aortic adenopathy: patterns of failure
and opportunities for cure.
Corn BW, Lanciano RM, Greven KM, Schultz DJ, Reisinger SA, Stafford PM, Hanks GE Int
J Radiat Oncol Biol Phys 1992;24(2):223-7
Hospital of the University of Pennsylvania, Department of Radiation Oncology, Philadelphia
19104.
PURPOSE: To examine the outcome of patients with advanced endometrial cancer whose
para-aortic involvement was diagnosed pathologically or lymphographically. METHODS AND
MATERIALS: Fifty patients from four institutions were treated between 1959 and 1990 with
preoperative, post-operative, and primary radiotherapy. Para-aortic disease was diagnosed
pathologically in 26 patients and lymphographically in the remaining 24 patients.
Pathologically diagnosed patients underwent debulking of grossly involved nodes. All
patients received external beam treatment through pelvic and para-aortic portals. Median
prescribed dose to the pelvic and para-aortic fields was 50 and 47 Gy, respectively. Those
treated with primary or pre-operative irradiation also received intrauterine
brachytherapy. RESULTS: The actuarial 5-year disease-free survival
was 46% for all patients. Para-aortic failure was
significantly decreased among patients undergoing lymph node resection (13% versus 39%,
respectively). Relapse-free survival and pelvic control tended to improve among
patients receiving surgery plus irradiation in comparison to those treated by irradiation
alone. Distant metastases were most common among patients with high grade lesions.
CONCLUSIONS: Long-term disease-free survival is achievable in endometrial cancer patients
with para-aortic lymphadenopathy who are treated with extended-field radiotherapy. Cure is
mot attainable among patients with well differentiated, early clinical stage disease who
receive combined modality treatment. Survival and local failure are similar for
radiologically and pathologically diagnosed patients; however, para-aortic failure as a
component of local failure was increased in patients who did not undergo surgical
debulking of the adenopathy.
Whole abdominal radiotherapy versus combination chemotherapy with
doxorubicin and cisplatin in advanced endometrial carcinoma (phase III): Gynecologic
Oncology Group Study No. 122.
Randall ME, Spirtos NM, Dvoretsky P J Natl Cancer Inst Monogr
1995;(19):13-5
Department of Radiation Oncology, Indiana University Medical Center, Indianapolis 46202,
USA.
Although localized endometrial cancer is effectively treated with surgery and radiation
therapy, the treatment of advanced disease remains problematic. With increasing
utilization of primary surgical staging and therapy, the early identification of patients
with tumor spread beyond the uterus is becoming routine. The impact of adjuvant
radiotherapy and/or chemotherapy in these patients remains to be demonstrated. In several
institutions, whole abdominal radiation therapy has been used with some success as
adjuvant treatment in selected patients with advanced disease. The Gynecologic Oncology
Group (GOG) has completed a phase II trial of the whole abdominal radiotherapy in this
patient population. Although data analysis is not complete, the regimen employed appears
to be tolerable and shows some evidence of efficacy. In previous GOG trials, cisplatin and
doxorubicin have shown single-agent activity in patients with measurable, advanced
endometrial cancer. Subsequently, the response rate with the combination of cisplatin and
doxorubicin was found to be superior to that with doxorubicin alone. Because
approximately 30%-50% of patients with extrauterine disease have systemic failure, the
evaluation of combination chemotherapy with doxorubicin and cisplatin in the adjuvant
setting seemed warranted. The current ongoing prospective, randomized trial (GOG
No. 122) compares the survival and the progression-free interval and treatment failure
patterns in patients with endometrial carcinoma of stage III or IV with up to 2 cm of
residual disease when treated with either whole abdominal radiotherapy or a combination of
doxorubicin and cisplatin. The incidence and type of acute and late adverse events
observed with the two treatment regimens were determined and compared. |

{kind=link}
{kind=link}
{kind=link}