Current status of HIFU and
cryotherapy in prostate cancer--a review.
Aus. G. Eur Urol. 2006 Nov;50(5):927-34; discussion 934. Epub 2006
Jul 28.
OBJECTIVES: To evaluate the current status of high-intensity focused
ultrasound (HIFU) and cryosurgery as the primary treatment option in
patients with prostate cancer. METHOD: A MedLine search using specified
search terms was done on February 28, 2005. This search rendered 150 papers
related to HIFU and 566 papers related to cryosurgery. Very few of these
papers presented original outcome data and are included in the present
review. RESULTS: No controlled trial was available for analysis, and no
survival data were presented. No validated biochemical, surrogate end point
was available for any of the two therapies. HIFU showed progression-free
survival (based on prostate-specific antigen+/-biopsy data) of 63-87%
(projected 3- to 5-yr data), but median follow-up in the studies ranged from
12-24 mo. Negative postoperative biopsies was seen in 82-94% of patients.
Complications have been reduced by the combination of transurethral
resection of the prostate and HIFU.
Cryosurgery showed a progression-free survival of 36-92% (projected 1-7 yr
data), depending on risk groups and definition of failure. Negative biopsies
were seen in 72-87%, but no biopsy data were available for the currently
used third-generation cryotherapy machines. Complications seem to be lower
with the third-generation machines. CONCLUSIONS:
None of the evaluated therapies has
enough data available to support their use as an alternative to established
therapies (surgery, radiation) for localised prostate cancer. Until
further data become available, the use of both treatments should be
restricted to patients unfit for established therapies who still have the
need for local therapy.
Third-generation cryotherapy for
prostate cancer in the UK: a prospective study of the early outcomes in
primary and recurrent disease.
Creswell J, BJU Int. 2006;97:969
Sunderland Royal Hospital, Sunderland, UK.
OBJECTIVE: To present the
early results of the use of third-generation cryotherapy in primary and
recurrent prostate cancer at one UK centre. PATIENTS AND METHODS: Over a
14-month period 51 patients underwent cryotherapy for prostate cancer. In 31
patients cryotherapy was used as the primary treatment and in 20 as a
salvage treatment after radiotherapy or hormone ablation. Data were
collected prospectively and the median follow-up was 9 months. RESULTS: The
prostate-specific antigen (PSA) level decreased to <0.5 ng/mL in 79% of
patients undergoing primary treatment and in 67% of patients undergoing
salvage treatment. A higher Gleason grade and PSA levels were associated
with a poorer outcome. No patient developed a fistula, 4% developed urinary
retention requiring transurethral prostatectomy and 4% had persistent
incontinence. The rates of erectile
dysfunction were high (86%). The median inpatient stay was 2 days.
CONCLUSION: Early results suggest that cryotherapy offers a safe alternative
for primary and recurrent prostate cancer, particularly for older and less
fit patients. Long-term data are required to assess the durability of
response and the effect on survival.
Comparison of health-related quality of life and
prostate-associated symptoms after primary and salvage cryotherapy for prostate cancer.
Anastasiadis AG, Sachdev R, Salomon L, Ghafar MA, Stisser BC, Shabsigh R, Katz AE.
J Cancer Res Clin Oncol. 2003 Oct 21
Department of Urology, Columbia University Health Sciences
PURPOSE. Recent advances in cryosurgery of the prostate have led to
the ability to treat tumors successfully with decreased morbidity. The patients'
perspectives of this relatively new technique, however, have not yet been addressed. The
purpose of this study was to compare health related quality of life (QoL) as well as
prostate-associated symptoms in patients after primary and salvage cryoablation for
clinically localized prostate cancer using a self-administered questionnaire. METHODS. A
total of 131 consecutive patients who underwent cryoablation of the prostate between 1997
and 2001 were included in this confidential mailing study. The patients were either (a)
patients with localized prostate cancer with contraindications for radical surgery,
including patients refusing other forms of therapy, or (b) had locally recurrent prostate
cancer after failure of radiation therapy. All patients received 3 months of neoadjuvant
androgen deprivation therapy prior to cryosurgery and were surgically treated by the same
surgeon using an argon-based system. We used the EORTC QLQ-C30, a commonly used,
multidimensional instrument together with a supplementing, prostate-cancer-specific
module. RESULTS. Eighty-one of the 131 patients (response rate 62%) returned the
questionnaires. The two groups were comparable regarding age (mean age 72.8 vs 70.1 for
the primary and the salvage group, respectively; p=0.22). The overall QoL scores were high
in both groups. Primary cryotherapy patients fared significantly better regarding physical
( p=0.005) and social ( p=0.024) functioning compared with salvage cryotherapy patients. The most prominent prostate-related symptom in both patient groups was
sexual dysfunction, followed by urinary symptoms, which were significantly more severe in
the salvage group ( p=0.001). Incontinence rates were 5.9 and 10% in the primary and the
salvage group, respectively.
Severe erectile dysfunction was
reported in 86 and 90% of the primary and the salvage group, respectively.
CONCLUSIONS. The present study demonstrates that, in selected patients, cryotherapy is a
treatment option which has a functional outcome comparable to traditionally used prostate
cancer treatments. More information regarding QoL is necessary for appropriate patient
counseling and individual decision-making in the presence of various treatment
alternatives.
Serial histopathology results of salvage cryoablation for prostate
cancer after radiation failure.
Chin JL, Touma N, Pautler SE, Guram KS, Bella AJ, Downey DB, Moussa M.
J Urol. 2003 Oct;170(4 Pt 1):1199-202.
University of Western Ontario, London, Canada. JCHIN@LHSC.ON.CA
PURPOSE: There has been a paucity of long-term followup reports of cryoablation for
prostate cancer. In particular, little is known regarding the
long-term histological results following salvage cryoablation. We report serial
biopsy results of up to 43 months on 106 patients who underwent cryoablation after radical
radiotherapy failed. MATERIALS AND METHODS: A total of 110 cryoablation procedures were
done in 106 patients for biopsy proven, clinically localized radiation failure.
Postoperatively transrectal ultrasound guided biopsy (usually 4 cores) was done at
approximately 3, and/or 6, 12 and 24 months, and thereafter as indicated by prostate
specific antigen, which was measured every 6 months. RESULTS: Of 818
biopsy cores a total of 23 (2.8%) from 15 patients (14.2%) were positive. Of the
positive cores 73.9% were found within year 1 following cryoablation. Residual viable
prostate glands and stroma were found in 42.4% and 27.4% of patients, respectively, at
various time points. The frequency of various histological features, the most common being
necrosis and fibrosis, was tabulated from the serial biopsy histology reports.
CONCLUSIONS: The results of serial biopsies have improved our understanding of the
histopathological changes as well as the capabilities and limitations of salvage
cryoablation. The biopsy positivity rate is acceptable, although the finding of persistent
viable prostatic tissue in a substantial proportion of patients implies that vigilant
long-term followup is mandatory.
Cryosurgery for prostate cancer.
Fahmy WE, Bissada NK. Arch Androl. 2003 Sep-Oct;49(5):397-407.
Medical University of South Carolina, Charleston, South Carolina, USA.
Choice of management for patients with prostate cancer is influenced by patient and
disease characteristics and life expectancy. Management options include expectance
(watchful waiting), radical prostatectomy, external beam radiotherapy, brachytherapy, and
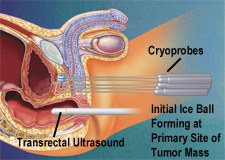
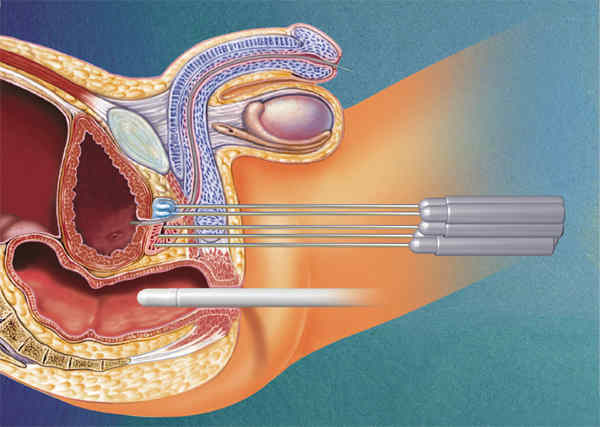
cryosurgical ablation of the prostate (CSAP). The role of
cryotherapy in the management of prostate cancer is still evolving. Continued
research has allowed the introduction of efficient and safe cryosurgical equipment
exemplified by the current third-generation cryosurgical machines. CSAP can be performed
in an ambulatory surgery setting or as inpatient surgery with overnight stay. The
procedure is performed under continuous ultrasonic monitoring. Mature data from the use of
second-generation cryosurgical equipment indicate that CSAP is an effective therapeutic
modality for managing patients with prostate cancer. Current data
with the third-generation cryosurgical equipment are not mature. However, the favorable
side effect profile and the good early responses seem to indicate that this modality will
have a prominent role in the management of patients with prostate cancer.
Salvage cryotherapy using an argon based system for locally
recurrent prostate cancer after radiation therapy: the Columbia experience.
Ghafar MA, J Urol. 2001 Oct;166(4):1333-7
Department of Urology, College of Physicians and Surgeons of Columbia University, New
York, New York, USA.
PURPOSE: Cryosurgical ablation of the prostate has been reported as potential treatment
for radioresistant clinically localized prostate cancer. We report our experience with the
safety and efficacy of salvage cryosurgery using the argon based CRYOCare system
(Endocare, Inc, Irvine, California). MATERIALS AND METHODS: Between October 1997 and
September 2000, 38 men with a mean age of 71.9 years underwent salvage cryosurgery for
recurrent prostate cancer after radiation therapy failed. All patients had biochemical
disease recurrence, defined as an increase in prostate specific antigen (PSA) of greater
than 0.3 ng./ml. above the post-radiation PSA nadir. Subsequently prostate biopsy was
positive for cancer. Pre-cryosurgery bone scan demonstrated no evidence of metastatic
disease. In addition, these patients received 3 months of neoadjuvant androgen deprivation
therapy before cryotherapy. RESULTS: The PSA nadir was 0.1 or less, 1 or less and greater
than 1 ng./ml. in 31 (81.5%), 5 (13.2%) and 2 (5.3%) patients, respectively. Biochemical recurrence-free survival calculated from Kaplan-Meier
curves was 86% at 1 year and 74% at 2 years. Reported complications included rectal pain
in 39.5% of cases, urinary tract infection in 2.6%, incontinence in 7.9%, hematuria in
7.9% and scrotal edema in 10.5%. The rate of rectourethral fistula, urethral sloughing and
urinary retention was 0%. CONCLUSIONS: Our study supports cryosurgery of the prostate as
safe and effective treatment in patients in whom radiation therapy fails. Using the
CRYOCare machine resulted in a marked decrease in complications.
Treatment of organ confined prostate cancer with third generation
cryosurgery: preliminary multicenter experience.
Han KR, .J Urol. 2003 Oct;170(4 Pt 1):1126-30.
University of California Los Angeles, USA.
PURPOSE: Cryosurgical ablation of the prostate is 1 approach to the treatment of localized
prostate cancer. Third generation cryosurgery uses gas driven probes that allow for a
decrease in probe diameter to 17 gauge (1.5 mm). The safety, morbidity and preliminary
prostate specific antigen (PSA) results of 122 cases are reported. MATERIALS AND METHODS:
A total of 106 patients have undergone percutaneous cryosurgery using a brachytherapy
template with at least 12 months of PSA followup. Immediate and delayed morbidities were
evaluated. PSA results at 3 and 12 months were recorded, and failure was defined as the
inability to reach a nadir of 0.4 ng/ml or less. RESULTS: Complications
in patients undergoing primary cryosurgery included tissue sloughing (5%), incontinence
(pads, 3%), urge incontinence/no pads (5%), transient urinary retention (3.3%) and rectal
discomfort (2.6%). There were no cases of fistulas or infections. Postoperative
impotence was 87% in previously potent patients. For patients who underwent salvage
cryosurgery there were no fistulas reported and 2 (11%) patients required pads after
salvage cryosurgery. A total of 96 (81%) patients achieved a PSA nadir of 0.4 ng/ml or
less at 3 months of followup, while 79 of 106 (75%) remained free from biochemical
recurrence at 12 months. A total of 42 (78%) low risk patients (Gleason score 7 or less
and PSA 10 or less) remained with a PSA of 0.4 ng/ml or less at 12 months of followup,
compared to 37 (71%) high risk patients. All patients were discharged within 24 hours.
CONCLUSIONS: After a followup of 1 year 3rd generation
cryosurgery appears to be well tolerated and minimally invasive. The use of
ultrathin needles through a brachytherapy template allows for a simple percutaneous
procedure and a relatively short learning curve. A prospective multicenter trial is
ongoing to determine the long-term efficacy of this technique.
Incomplete glandular ablation after salvage cryotherapy for
recurrent prostate cancer after radiotherapy.
Izawa JI, .Int J Radiat Oncol Biol Phys. 2003 Jun 1;56(2):468-72.
Department of Urology, The University of Texas M. D. Anderson Center, Houston, TX 77030,
USA.
PURPOSE: To determine the clinical variables associated with inadequate salvage
cryotherapy and to correlate the disease-free survival rates associated with biopsy
results in prostate cancer (CaP). METHODS AND MATERIALS: Between July 1992 and January
1995, 150 patients underwent salvage cryotherapy for locally recurrent CaP. Biopsy
specimens were examined for the presence of cancer cells and normal or atypical glands,
all of which were considered evidence of inadequate cryotherapy. Clinical variables, as
predictors of biopsy results, were evaluated with univariate and multivariate analyses.
The impact of the biopsy results on disease-free survival was also determined. RESULTS:
The number of cryoprobes and freeze-thaw cycles correlated with inadequate cryotherapy (p
= 0.037 and p = 0.0022, respectively). The number of freeze-thaw cycles was an independent
predictor of inadequate cryotherapy (p = 0.003). The finding of cancer cells in the biopsy
specimens was the only histopathologic variable that affected disease-free survival (p =
0.016). CONCLUSION: Complete ablation of the prostate gland and
tumor is difficult to achieve with salvage cryotherapy. To optimize for
complete ablation, salvage cryotherapy should include at least two freeze-thaw cycles and
a minimum of five cryoprobes. The finding of atypical or normal epithelial tissue in
biopsy specimens after salvage cryotherapy is not predictive of biochemical failure.
Local tumor control with salvage cryotherapy for locally recurrent
prostate cancer after external beam radiotherapy.
Izawa JI, J Urol. 2001 Mar;165(3):867-70.
Department of Urology, University of Texas M. D. Anderson Center, Houston, Texas, USA.
PURPOSE: We identified variables associated with a positive prostate biopsy after salvage
cryotherapy in patients in whom initial external beam radiotherapy for prostate cancer
failed to improve our cryotherapy technique, optimize local control and improve our
patient selection criteria for salvage cryotherapy. MATERIALS AND METHODS: Between July
1992 and January 1995, 145 patients underwent salvage cryotherapy. Post-cryotherapy
sextant prostate biopsies were performed in 107 cases. We evaluated certain variables on
univariate and multivariate analysis as predictors of a positive biopsy after cryotherapy,
including the type of previous therapy, tumor stage and grade at initial diagnosis,
prostate volume, pre-cryotherapy prostate specific antigen (PSA), number of positive
biopsy cores before cryotherapy, PSA nadir after cryotherapy, stage and grade of local
recurrence, number of cryoprobes, number of freeze-thaw cycles and use of a urethral
warming catheter during cryotherapy. RESULTS: Biopsies were
positive in 23 cases (21%) after salvage cryotherapy. Variables associated with
a positive biopsy on univariate analysis were initial stage, precryotherapy PSA, PSA nadir
after cryotherapy, number of cryoprobes, number of freeze-thaw cycles and a history of
chemotherapy (p = 0.005, 0.027, 0.001, 0.009, 0.018 and 0.008, respectively). Variables
that remained associated with a positive biopsy on multivariate analysis were the number
of probes used and post-cryotherapy PSA nadir (p = 0.013 and 0.019, respectively).
CONCLUSIONS: Patients with initial clinical stage T1-2N0M0 disease and PSA no more than 10
ng./ml. have a higher rate of negative biopsies after salvage cryotherapy. Therefore, they
are better candidates for salvage cryotherapy for locally recurrent prostate
adenocarcinoma after external beam radiotherapy. To optimize the potential for local
control the technique of salvage cryotherapy should include 2 freeze-thaw cycles and a
minimum of 5 cryoprobes. Detectable PSA after salvage cryotherapy is a strong predictor of
local failure.
Patient selection for salvage cryotherapy for locally recurrent
prostate cancer after radiation therapy.
Pisters LL, .J Clin Oncol. 1999 Aug;17(8):2514-20.
Department of Urology, The University of Texas M. D. Anderson Cancer Center, Houston, TX
77030, USA. lpisters@mdanderson.org
PURPOSE: Our objective was to identify clinical pretreatment factors associated with early
treatment failure after salvage cryotherapy. PATIENTS AND METHODS: Between 1992 and 1995,
145 patients underwent salvage cryotherapy for locally recurrent adenocarcinoma of the
prostate. Treatment failure was defined as an increasing postcryotherapy serial
prostate-specific antigen (PSA) level of more than or equal to 2 ng/mL above the
postcryotherapy nadir or as a positive posttreatment biopsy. We evaluated the following
factors as predictors of treatment failure: tumor stage and grade at initial diagnosis,
type of prior therapy, stage and grade of locally recurrent tumor, number of positive
biopsy cores at recurrence, and precryotherapy PSA level. RESULTS: Among patients with a prior history of radiation therapy only, the 2-year
actuarial disease-free survival (DFS) rates were 74% for patients with a precryotherapy
PSA less than 10 ng/mL and 28% for patients with a precryotherapy PSA more than 10 ng/mL,
P <.00001. The DFS rates were 58% for patients with a Gleason score of less than or
equal to 8 recurrence and 29% for patients with a Gleason score greater than or equal to 9
recurrence, P <.004. Among patients with a precryotherapy PSA less than 10
ng/mL, DFS rates were 74% for patients with a prior history of radiation therapy only and
19% for patients with a history of prior hormonal therapy plus radiation therapy, P
<.002. CONCLUSION: Patients failing initial radiation therapy with a PSA more than 10
ng/mL and Gleason score of the recurrent cancer more than or equal to 9 are unlikely to be
successfully salvaged. Patients failing initial hormonal therapy and radiation therapy are
less likely to be successfully salvaged than patients failing radiation therapy only.
|

{kind=link}