 |
PET - CT Scans of the Breast
|
|
PET - CT Scans of the Breast
|
![]()
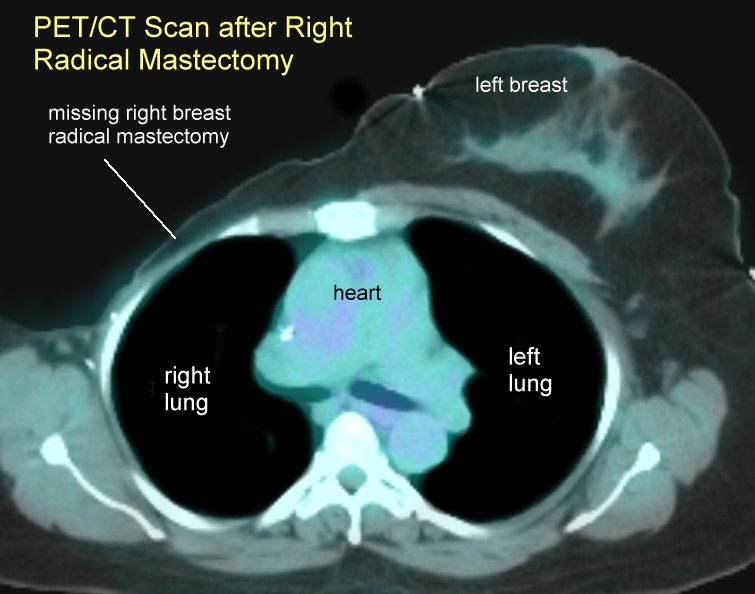
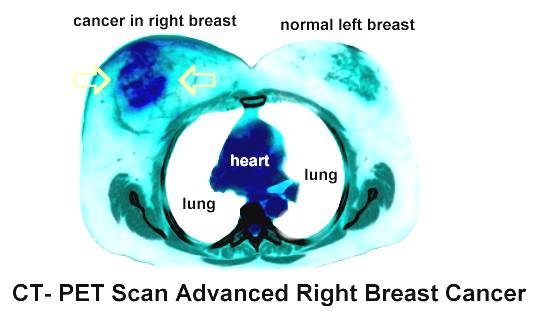
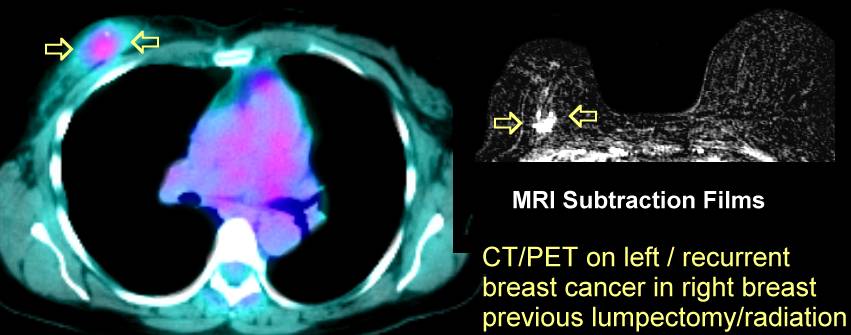
| PET imaging using 18-FDG has demonstrated potential in the
differentiation of benign from malignant breast lesions. One of the benefits of PET
imaging is that it is not affected by the density of breast tissue. Image quality is also
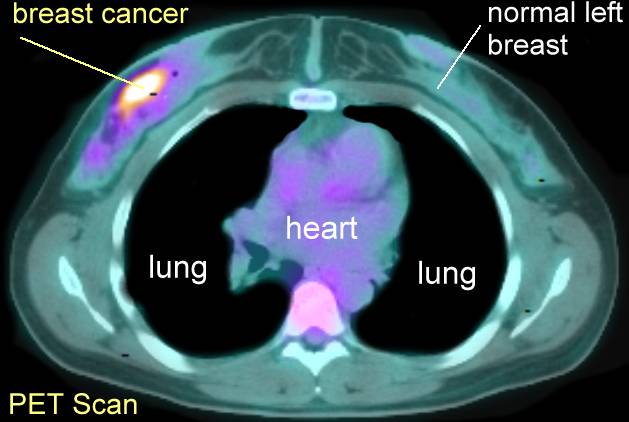
not impaired by prior surgery, prior XRT, or breast implants. Reported sensitivities for FDG PET range from 64% to
96%, and specificity's from 75% to 100% . In a meta-analysis of 606 patients, PET had a
sensitivity of 88%, and a specificity of 79% for differentiating benign from malignant
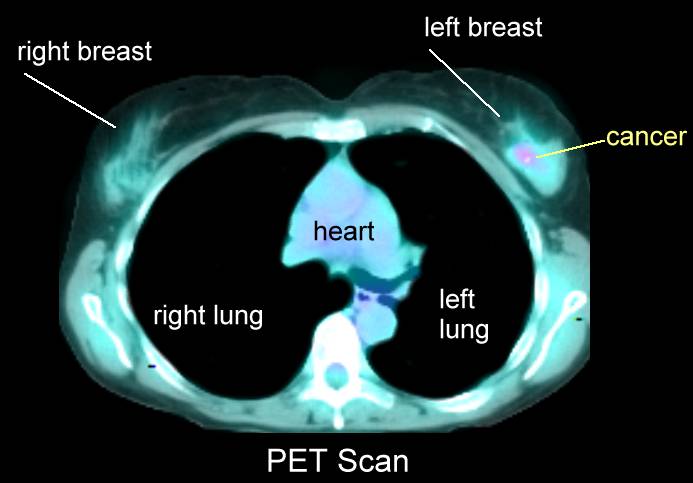
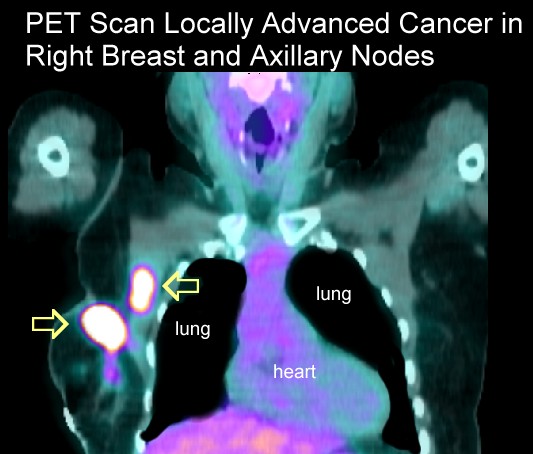
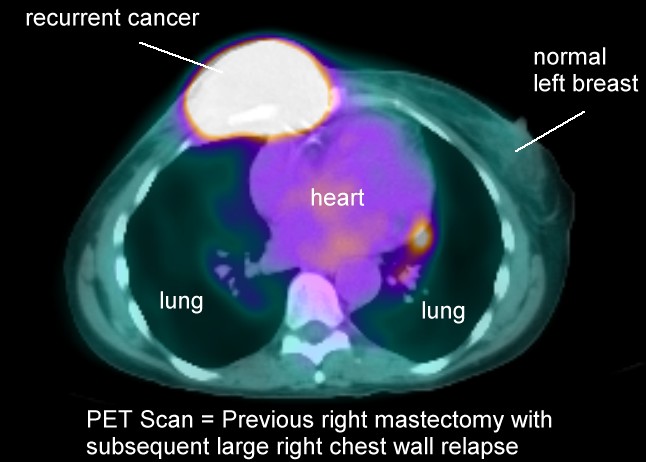
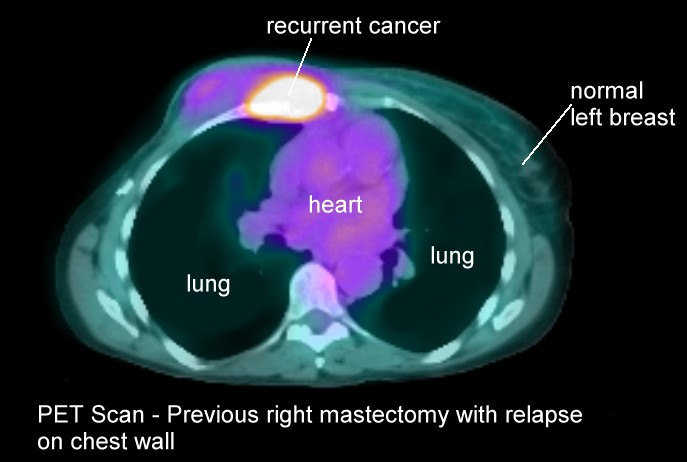
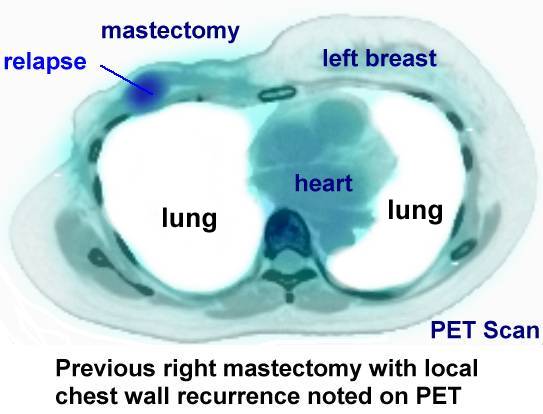
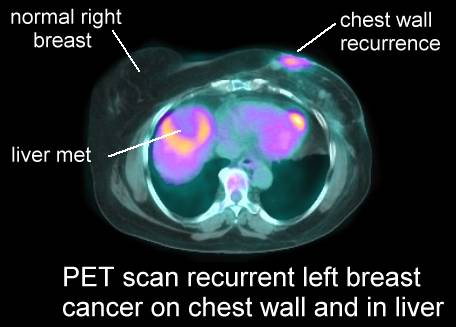
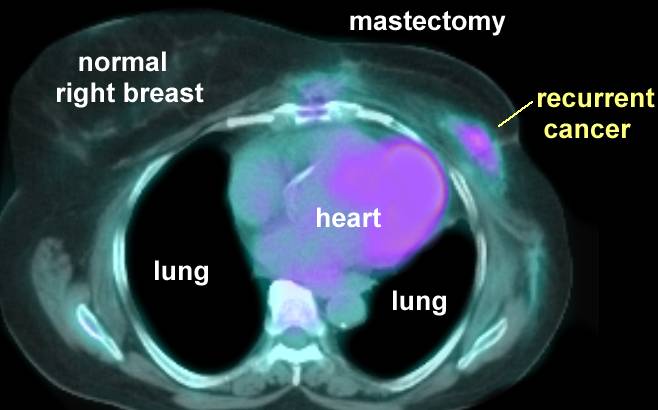
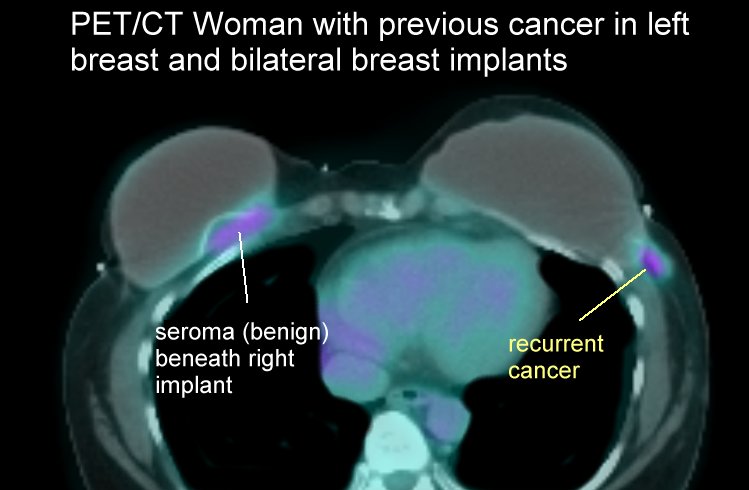
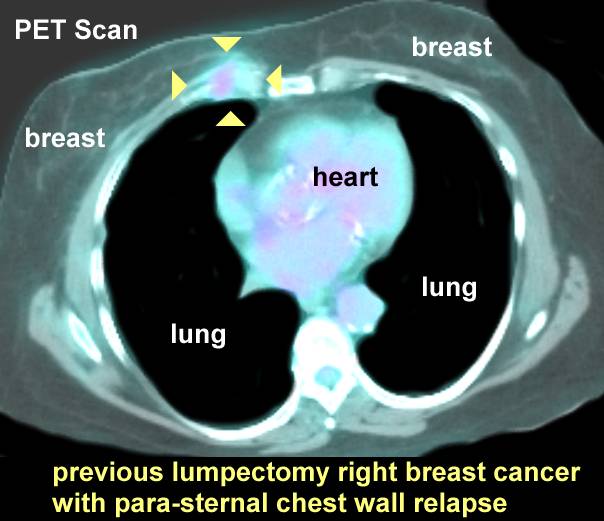
lesions. The primary limitation of FDG-PET imaging for evaluation of breast carcinoma is its inability to detect small lesions (under 1 cm in size) due to partial volume effects and natural tracer accumulation in the breast which may obscure low uptake lesions. The sensitivity of PET is only 25% for tumors smaller than 1 cm, but can be as high as 84% for tumors between 1-2 cm Although the sensitivity is generally higher for lesions greater than 1 to 2 cm in size, even larger lesions may not necessarily demonstrate tracer accumulation (up to 20% of lesions between 2 to 5 cm in size may be falsely negative on PET FDG imaging). A larger percentage of invasive lobular carcinomas are not detected (65% in one study), possibly due to low tumor cell density, its infiltrative nature, and low metabolic activity. Tubular carcinoma and ductal carcinoma in situ also show less FDG accumulation and these lesions may not be reliably distinguished from normal breast tissue. None-the-less, PET imaging may be useful in a carefully selected subgroup of patients with inconclusive conventional imaging procedures. For lesions of sufficient size, a positive PET scan carries a high positive predictive value that the lesion is breast cancer. False-positive findings are also infrequent (about 5% of benign lesions will demonstrate tracer uptake). False positive exams have been reported in association with inflammation (mastitis) fibroadenomas (about 10% accumulate FDG, and ductal adenomas. FDG PET imaging can also aid in the detection of metastases to lymph nodes and other unsuspected sites in the body. Pre-operative determination of node status is essential as clinical evaluation is usually inaccurate. Up to 40% of patients with a clinically negative exam demonstrate the presence of metastases at histologic examination. Conversely, 40% of patients clinically suspected of having lymph node metastases, are found to be negative on histologic review. Reported PET sensitivities for locoregional nodal metastases range from 50% to 100%. Specificity for the detection of axillary nodal metastases ranges from 86% to 92%. Lower sensitivities for axillary nodal metastases can be expected for metastatic foci smaller than 1 cm in diameter and those with micrometastases. Consequently, a negative FDG PET exam should not preclude lymphoscintigraphy and axillary node dissection [4]. PET imaging, however, can uncover nodal disease in sites unrecognized by conventional imaging. FDG PET imaging has been shown to be superior to conventional imaging for the detection of mediastinal and internal mammary nodal metastases (sensitivity 85% versus 54% for CT). The identification of unsuspected metastases in the mediastinal and internal mammary nodal regions has a significant impact on patient management and long term prognosis. Patients with positive internal mammary nodes have a significantly worse prognosis for both disease-free and overall survival. Management of these patients may require extending the radiation field to include these nodes (which can result in survival benefit) or initiating a more aggressive chemotherapeutic regimen. PET imaging has been shown to be superior to bone scan for the detection of osteolytic bone metastases. FDG PET imaging can significantly impact on patient management- particularly in patients with suspected advanced stage disease. PET findings can result in a change in the patients clinical stage in up to 36% of patients (28% upstaged, 8% downstaged). Unsuspected sites of nodal or distant metastases can be found in up to 20% of patients. In one prospective study of 48 patients with locally advanced breast cancer, PET imaging detected unsuspected distant metastatic disease in 8% of patients. Equally important is the fact that the patient's clinical management can be changed in up to 58% of patients based upon the results of the PET study. Evaluation of tumor recurrence: The clinical course of patients with recurrent breast cancer varies and is largely dependent on the extent of metastatic disease and the biological aggressiveness of the tumor. Accurate staging is critical for therapeutic planning. Unfortunately, previous surgery and radiation therapy can result in scarring that can complicate the evaluation for locoregional recurrence of breast cancer- particularly in the axillary region. Exploratory surgery of the axilla has been used to confirm or exclude recurrent disease, but can yield inconclusive results due to sampling error. Furthermore, early distant metastatic disease may not be suspected clinically or may not be appreciated on conventional imaging. FDG PET has demonstrated usefulness in discriminating tumor recurrence from post-operative and post-radiation changes in the breast and PET imaging has also been shown to add incremental information to conventional imaging studies in defining disease extent. Locoregional recurrence: Local or regional recurrence of breast cancer occurs after initial diagnosis and treatment in 7-30% of patients. After conservative surgical resection and radiation, the most common sites of locoregional recurrence are the breast, the skin of the breast, chest wall, and local nodal basins. In these patients, risk factors for locoregional recurrence include positive margins at surgery, age under 40 years, and tumors containing an extensive intraductal component. FDG PET has a reported sensitivity of up to 100% for the detection of locoregional recurrence. For patients with suspected or known locoregional recurrence, under consideration for aggressive local treatment, PET imaging findings can significantly affect patient management. By detecting unsuspected sites of disease, planned therapy can be altered in up to 44% of patients. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}