|
also the see review article from the Cleveland
Clinic here.
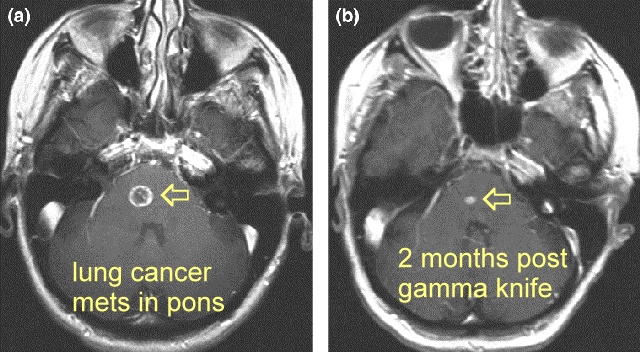
Stereotactic radiosurgery
for brainstem metastases: Survival, tumor control, and patient outcomes |
|
| Stereotactic radiosurgery is proven
to provide local tumor control and provide survival benefit in combination with WBRT for
selected patients with brain metastases. However, few data are
available to evaluate the effectiveness of SRS for patients with metastases to the
brainstem. In fact, despite the fact that SRS is commonly employed to manage
patients with brainstem metastases, some question the value of SRS for this patient group.
Suki and colleagues reviewed the MD Anderson Cancer Center
experience and found complications in 37% of patients after SRS for brainstem metastases;
this is in sharp contrast to our experience with only 1 patient (5%) of 22 having a
significant complication. This discrepancy may be partially explained by how Suki and
colleagues accounted for complications including events such as tumor failures, death,
seizures, and deep venous thromboses under the category of complications. Two previous series described the use of SRS in the management of patients with brainstem metastasis and had a more favorable experience. Both Huang (Pittsburgh) and Fuentes (Marseilles) e) noted high local control rates (92–95%) similar to our experience. The median tumor margin dose in Huang et al. was 16 Gy compared with 19.6 Gy in the report by Fuentes et al. This difference in radiosurgical dosing likely relates to the number of patients that either underwent prior or else planned WBRT in conjunction with SRS. Twenty-four of 26 patients (92%) underwent WBRT in the Pittsburgh study (6), whereas only 6 of 28 (21%) patients received WBRT in the Marseilles study. Survival times and complication rates were also quite similar in these articles compared to our results. The median survival time observed after SRS ranged from 8.5 to 12 months in these two articles. Similar to brain metastasis patients with tumors not located in the brainstem, the most important predictor of survival after SRS is the extent and management of extracranial disease The results in our small series, of a median survival of 8.5 months, local control of 100%, and a 5% incidence of a radiation-related complication is not remarkably different than most radiosurgical series of brain metastasis patients in the literature. However, one should not assume there is no difference in the outcomes after SRS for brainstem compared to cerebral metastases, because this is obviously a highly selected population with only 22 patients with brainstem metastases treated over a 14-year period at the Mayo Clinic. Nonetheless, SRS should be strongly considered for patients with brainstem metastases, especially those patients with limited systemic disease and good performance status, noting SRS provides better local control than WBRT and concerns regarding significant morbidity and mortality associated with microsurgery for brainstem metastases. It should be emphasized that the treatment of brainstem metastases larger than the median size described in this study (0.9.mL), and especially those larger than 1.5 mL, should be considered for a dose reduction relative to the SRS doses used in this sample of patients. Similarly, radiosurgery delivered with less conformal methods than the Leksell Gamma Knife should also consider dose reduction or sending the patient to an appropriate facility capable of highly conformal radiosurgery. |
| Stereotactic radiosurgery
for brainstem metastases. Huang CF,
Kondziolka D, Flickinger JC, et al..J Neurosurg. 1999;91:563–568 Brainstem metastases portend a dismal prognosis. Surgical resection is not part of routine management and radiation therapy has offered little clinical benefit. Radiosurgery provides a safe and effective treatment for many patients with brain metastasis, but its role in the brainstem has not been evaluated. In this study the authors examine the role of radiosurgery in the treatment of brainstem metastases. METHODS: The authors reviewed the outcomes after stereotactic radiosurgery in 26 patients with 27 brainstem metastases. Tumor locations included the pons (21 tumors) and midbrain (six tumors): 14 patients had additional tumors in other locations. Twenty patients presented with brainstem signs. The median dose to the tumor margin was 16 Gy (range 12-20 Gy). Twenty-four patients received fractionated whole-brain radiation therapy (WBRT) and 12 underwent additional chemotherapy or immunotherapy. The median follow-up time in these patients was 9.5 months (range 1-43 months). After radiosurgery, the local control rate in brainstem tumors was 95%. In one patient in whom the tumor initially decreased in size, tumor enlargement was seen 7 months later. The median survival time was 11 months after diagnosis and 9 months after radiosurgery. Thirteen patients improved, 10 were stable, and three deteriorated. Eventually, 22 patients died, 18 of progression of their extracranial disease, three of new tumor growth (including one hemorrhage into a new brain metastasis), and one of extracranial disease plus new brain tumor growth. CONCLUSIONS: Although they have slightly lower than the expected survival rates of patients with nonbrainstem tumors, patients with brainstem metastases may achieve effective palliation after stereotactic radiosurgery and WBRT. Brainstem metastases: Management using Gamma-Knife radiosurgery. Fuentes S, Delsanti C, Metellus P, et al. Neurosurgery. 2006;58:37–40. Neurosurgical Service, Timone University Hospital Center, Marseille, France. sfuentes@ap-hm.fr OBJECTIVE: Brainstem metastasis is an uncommon complication of systemic cancer, generally considered to have a highly unfavorable prognosis. Surgical risks are high and standard radiation or chemotherapy have little effect. The purpose of this study is to evaluate our experience using Gamma Knife radiosurgery (GKRS) for the management of brainstem metastasis. METHODS: Between July 1992 and March 2001, we treated 28 patients with brainstem metastasis using GKRS. Lesions were located in the pons in 17 patients, midbrain in nine, and medulla oblongata in two. At time of the radiosurgery, eight patients presented with another supratentorial metastasis. The most frequent primary tumor site was the lung (13 cases) followed by the melanoma in four cases, the kidney in two, and other locations in six. Only six patients underwent fractionated whole-brain radiation therapy. Mean marginal radiation dose for GKRS was 19.6 Gy (range, 11-30). Mean maximum diameter was 17.2 mm (range, 10-30). RESULTS: No GKRS-related morbidity was observed. Local tumor control was achieved in 92% of patients. Twenty-six patients have died. Death was related to the progression of the brainstem lesion in two cases. Mean and median survival after GKRS were 10.2 and 12 months, respectively. Follow-up periods in the two surviving patients were 12 and 13 months. CONCLUSION: The results of this small series demonstrate that GKRS can be a valuable modality for safe and effective management of brain stem metastasis. Owing to the high risk of surgical resection and low efficacy of medical treatment, radiosurgery can be proposed upfront. |