|
|
|
|
|
|
 |
 |
Bone
Metastases
Bone metastases occur in 30-70% of patients with cancer, cancer of the breast and
prostate account for the majority of bone metastases, and the lungs, kidneys, and thyroid
are relatively frequent sources. Metastatic disease to bone develops in two thirds of
carcinomas of the breast and in 50% of carcinomas of prostate. Twenty-five percent of
tumors in the lungs and kidneys produce skeletal metastases, but skeletal metastases occur
in no more than 10% of all other malignancies. Carcinomas of the gastrointestinal tract
(esophagus, stomach, pancreas, and colon) and the genital tract (ovaries, uterus, cervix,
and testicles), although common, rarely metastasize to bone. Likewise, sarcomas rarely
metastasize to bone. By percent the most common cancers with bone metastases are breast
(50%) prostate (17%) and lung (11%.)
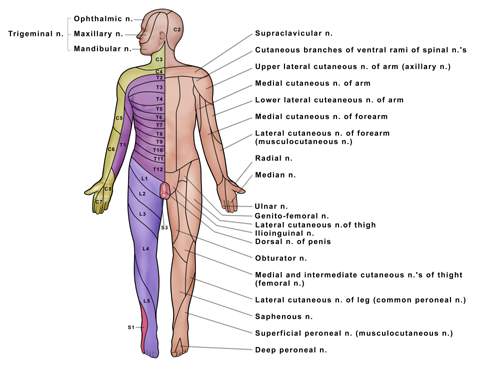
The most common bones involved are vertebra (69%) pelvis (41%) femur (25%) skull (14%) and upper extremity (10 -15%.) The pain may be local or radiate alone the course of the nerves (see dermatome chart, and other dermatome charts a, b, c, d.)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The treatment of bone metastases starts with treating the underlying cancer. If the cancer can be successfully treated with hormonal therapy (e.g. breast or prostate cancer) or chemotherapy (e.g. myeloma) then this should be started. Also most patients benefit from bisphosphonate durgs (Aredia or Zometa) which promote bone healing. Radiation is used for primarily two reasons: if the lesion is painful or showing signs of significant bone destruction. As noted below radiation is usually quite successful in relieving pain and will also promote bone healing by killing the cancer in the bone and allowing normal bone regrowth to occur. If the bone is severely weakened it may be prudent to perform surgical stabilization prior to radiation (see section on surgery.) If the cancer is extremely widespread then isotope therapy (which treats all the bones) my be better than local radiation (see section on isotopes, samarium or strontium.)