|
Radiation for Cancer
of the Anal Canal anatomy contouring here or here Based on the
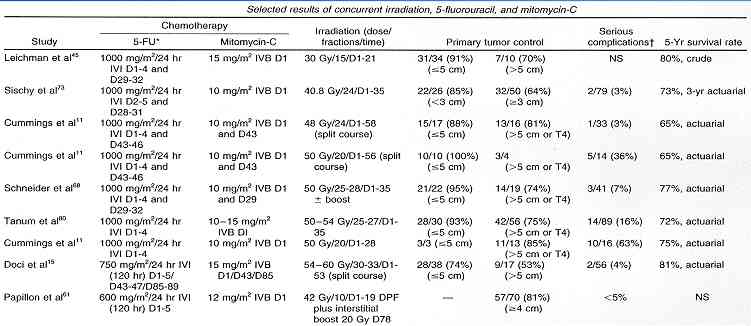
studies below, it appears that radiation combined with chemoRx (5FU + Mitomycin see
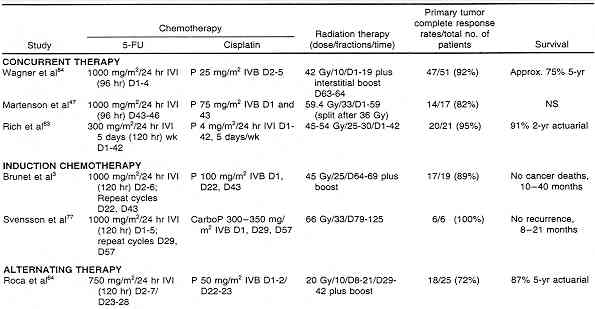
data, or perhaps new regimens that contain Platinol, see
data produce the best results. Other recent data is here.
(Cisplatin may be less toxic than Mitomycin, see MD Anderson study.) The proper
dose of radiation is unknown. The original trials (Nigro) used low doses (30Gy) but
the standard has become 45-50Gy plus or minus a boost dose (9Gy if + bx or in some
protocols a routine dose of 15-20Gy is added.) See recent MDA paper on technique here. The approach at the U of Florida seems quite reasonable. (The current NCI page notes: "The optimal dose of radiation with concurrent chemotherapy to optimize local control and minimize sphincter toxic effects is under evaluation but appears to be in the 45 Gy to 60 Gy range.") See details of RTOG anal trial 9811 and RTOG 0529 and the results here. Typical results using modern chemoradiation with IMRT are here and here. Some of the older studies are here |

{kind=link}
{kind=link}