Postoperative
Irradiation with or without Concomitant Chemotherapy for Locally Advanced Head and Neck
Cancer
Jacques Bernier, for the European Organization for Research and
Treatment of Cancer Trial 22931
Methods After undergoing surgery
with curative intent, 167 patients were randomly assigned to receive
radiotherapy alone (66 Gy over a period of 6 1/2 weeks)
and 167 to receive the same radiotherapy regimen combined with 100 mg of
cisplatin per square meter of body-surface area on days 1, 22, and 43 of the
radiotherapy regimen.
After a median follow-up of 60 months, the rate of
progression-free survival was significantly higher in the combined-therapy
group than in the group given radiotherapy alone (P=0.04 by the log-rank test;
hazard ratio for disease progression, 0.75; 95 percent confidence interval,
0.56 to 0.99), with 5-year Kaplan–Meier estimates
of progression-free survival of 47 percent and 36 percent, respectively.
The overall survival rate was also significantly higher
in the combined-therapy group than in the radiotherapy group (P=0.02 by the
log-rank test; hazard ratio for death, 0.70; 95 percent confidence
interval, 0.52 to 0.95), with five-year Kaplan–Meier estimates of overall survival of 53 percent and 40 percent, respectively.
The cumulative incidence of local or regional relapses was significantly lower
in the combined-therapy group (P=0.007). The estimated five-year cumulative
incidence of local or regional relapses (considering death from other causes
as a competing risk) was 31 percent after radiotherapy and 18 percent after
combined therapy. Severe (grade 3 or higher) adverse effects were more frequent
after combined therapy (41 percent) than after radiotherapy (21 percent,
P=0.001); the types of severe mucosal adverse effects were similar in the two
groups, as was the incidence of late adverse effects.
Conclusions Postoperative concurrent administration of high-dose cisplatin
with radiotherapy is more efficacious than radiotherapy alone in patients with
locally advanced head and neck cancer and does not cause an undue number of
late complications. NEJM 2004;350:1945 |
Postoperative
Concurrent Radiotherapy and Chemotherapy for High-Risk Squamous-Cell Carcinoma of the Head
and Neck
Jay S. Cooper RTOG 9501, ECOG R9501, and SWOG 9515
Between September 9, 1995, and April 28, 2000, 459 patients were enrolled.
After undergoing total resection of all visible and palpable disease, 231
patients were randomly assigned to receive radiotherapy alone (60 to 66 Gy in 30 to 33 fractions over a period of 6 to 6.6
weeks) and 228 patients to receive the identical treatment plus concurrent
cisplatin (100 mg per square meter of body-surface area intravenously on days
1, 22, and 43).
Results After a median follow-up of 45.9 months, the rate of local
and regional control was significantly higher in the combined-therapy group
than in the group given radiotherapy alone (hazard ratio for local or regional
recurrence, 0.61; 95 percent confidence interval, 0.41 to 0.91; P=0.01).
The estimated two-year rate of local and regional control was 82 percent in the
combined-therapy group, as compared with 72 percent in the radiotherapy group.
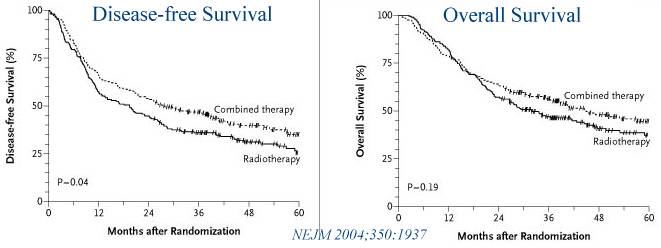
Disease-free survival was significantly longer
in the combined-therapy group than in the radiotherapy group (hazard ratio for
disease or death, 0.78; 95 percent confidence interval, 0.61 to 0.99; P=0.04),
but overall survival was not (hazard ratio for death, 0.84; 95
percent confidence interval, 0.65 to 1.09; P=0.19). The incidence of acute
adverse effects of grade 3 or greater was 34 percent in the radiotherapy group
and 77 percent in the combined-therapy group (P<0.001). Four patients who
received combined therapy died as a direct result of the treatment.
Conclusions Among high-risk patients with resected head and neck
cancer, concurrent postoperative chemotherapy and radiotherapy significantly
improve the rates of local and regional control and disease-free survival. However, the combined treatment is associated with a substantial increase in
adverse effects.
NEJM 2004;350:1937 |