|
|
Refining
Multimodal Therapy for Rectal Cancer |
Mesorectal Excision |
|
|
Refining
Multimodal Therapy for Rectal Cancer |
Mesorectal Excision |
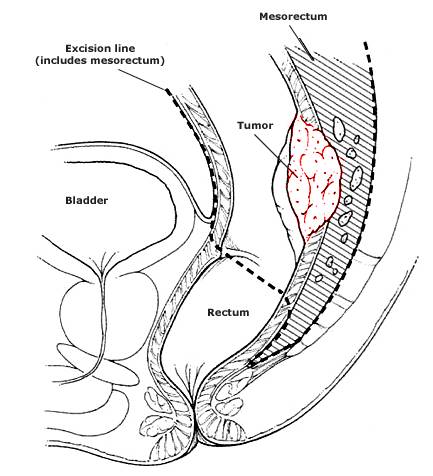
In Germany, the introduction of a specialized technique,
total
mesorectal excision, has reduced local recurrence rates from 39 to 10
percent. Total mesorectal excision was developed after the recognition that
discontinuous tumor deposits are often present in the lymphovascular tissue
that surrounds the rectum (the mesorectum); left in place, such residual
deposits are most likely the origin of local treatment failure (see picture
above.) Total mesorectal excision has evolved to become more consistent with
wide anatomical mesorectal excision, the essence of which is to use anatomical
planes to dissect the mesorectum under direct visualization, so that the fascia
propria is preserved with the rectal specimen for at least 4 cm distal to the
tumor. In summary: Preoperative adjuvant therapy
seems justified in patients who are known to have extensive local disease or
lymph-node involvement. For patients with early-stage disease, the following
strategy seems appropriate: perform surgery first and reserve adjuvant therapy
for those with pathological findings that confirm the presence of transmural
invasion or lymph-node involvement. Heidi Nelson, M.D..
Daniel J. Sargent, Ph.D. Mayo Clinic NEJM 2001;345:690
Preoperative Radiotherapy
Combined with Total Mesorectal Excision for Resectable Rectal Cancer
Ellen Kapiteijn, M.D. for the Dutch Colorectal Cancer Group NEJM
2001;345:638
We randomly assigned 1861 patients with resectable rectal cancer either to preoperative radiotherapy (5 Gy on each of five days) followed by total mesorectal excision (924 patients) or to total mesorectal excision alone (937 patients). The trial was conducted with the use of standardization and quality-control measures to ensure the consistency of the radiotherapy, surgery, and pathological techniques.
Results Of the 1861 patients randomly assigned to one of the two treatment groups, 1805 were eligible to participate. The overall rate of survival at two years among the eligible patients was 82.0 percent in the group assigned to both radiotherapy and surgery and 81.8 percent in the group assigned to surgery alone (P=0.84). Among the 1748 patients who underwent a macroscopically complete local resection, the rate of local recurrence at two years was 5.3 percent. The rate of local recurrence at two years was 2.4 percent in the radiotherapy-plus-surgery group and 8.2 percent in the surgery-only group (P<0.001).
Conclusions Short-term preoperative radiotherapy reduces the risk of local recurrence in patients with rectal cancer who undergo a standardized total mesorectal excision.
| Group | Surgery | Radiation + Surgery |
| all | 8.2% | 2.4% |
| procedure | ||
| low anterior | 7.3% | 1.2% |
| APR | 10.1% | 4.9% |
| Stage | ||
| I | 0.7% | 0.5% |
| II | 5.7% | 1.0% |
| III | 15% | 4.3% |
| IV | 23.8% | 10.1% |
![]()