 |
|
|
|
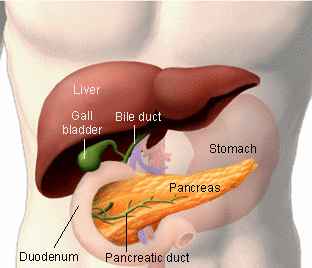
Clinical presentation Most exocrine pancreatic tumors (85%) are adenocarcinomas, usually of ductal origin. Other, rare histologic types include acinar cell, papillary and cystic neoplasm, and cystadenocarcinoma. Cystadenocarcinomas, which are usually large tumors at the time of presentation and have a greater propensity for occurring in the tail of the pancreas, should be recognized because they can be somewhat more indolent than ductal pancreatic carcinomas. Papillary and cystic neoplasms carry a very favorable prognosis and are usually cured by surgery. It is also important to distinguish exocrine tumors from neuroendocrine tumors of the pancreas, also known as islet cell carcinomas. These tumors often produce secretory products with associated clinical syndromes: Insulinomas cause intermittent hypoglycemic syndromes; gastrinomas produce increased gastrin production and secondary ulcers; glucagonomas cause hyperglycemia; and vasoactive intestinal peptidesecreting tumors (VIPomas) cause massive watery secretory diarrhea. Carcinoid tumors can usually be detected by urinary 5-hydroxyindole acetic acid levels, and, if functional, have symptoms of flushing and diarrhea. Patients with pancreatic cancer have pain sometime during the course of their disease but not always on initial presentation. If the tumor is located at the head of the pancreas, obstructive jaundice, with or without pain, may result. Tumors in the body or tail usually do not cause any symptoms until they have reached a larger size or a more advanced stage.. Evaluation Patients with suspected pancreatic tumors should be evaluated with a CT scan of the abdomen.However, endoscopic retrograde cholangiopancreatography (ERCP) has a greater sensitivity and specificity, which is further increased by obtaining cytologic brushings. It is especially useful for small lesions in the head of the pancreas and is indicated in cases with jaundice. CT scandirected needle biopsies of the pancreatic mass may also obtain confirmatory tissue but if there is coincident hepatic metastasis, a liver biopsy is often preferable. Sometimes the pathologic diagnosis can only be obtained via laparoscopy or laparotomy. Tumor markers such as CA19-9 and CEA are not diagnostic. CA19-9, in particular, can be elevated in benign conditions, and can be elevated in patients with malignancies other than pancreatic cancer.)Though an extremely high CA19-9 increase the likelihood of pancreas cancer if the images are suspicious as well see here.) Treatment Patients with tumors confined to the pancreas on CT scan without involvement of critical blood vessels (superior mesenteric artery, superior mesenteric vein, celiac axis) are potential candidates for surgical resection. Laparoscopic evaluation has a high rate of identification of peritoneal, hepatic, or other metastases that preclude resection, and should be done as an initial maneuver in all planned resections. The use of combined postoperative radiation therapy and chemotherapy has shown a survival advantage over observation alone in completely resected patients, but survival remains dismal with only 10% of these patients alive at 5 years. Patients with locally advanced disease may benefit from radiation therapy in conjunction with 5-FU. This may provide useful palliation, and rare long-term survivors have been seen. Because local radiation therapy in this site can cause significant morbidity, the role of radiation therapy should be carefully considered in patients with significant medical comorbidities or debilitation. An ERCP can be performed to attempt stent placement for bypass of biliary obstruction in patients with obstructive jaundice, or patients can be palliated surgically. Chemotherapy offers no substantial survival advantage in patients with advanced disease. The role of chemotherapy in the palliation of symptoms remains controversial. Multiple-agent chemotherapy has not been proved more effective when compared with single-agent 5-FU regimens [49]. More recently, gemcitabine has gained approval as a first-line treatment for metastatic pancreatic cancer. In a randomized trial against 5-FU, gemcitabine had a small but statistically significant improvement in median survival over 5-FU. Pain control in pancreatic cancer patients can include local interventions, such as celiac nerve blocks or epidural administration of analgesics. Patients also often require replacement of pancreatic enzymes to assist in the alleviation of associated gastrointestinal symptoms. |
{kind=link}
{kind=link}