|
|
|
|
|
|
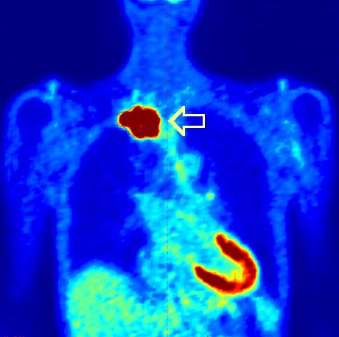
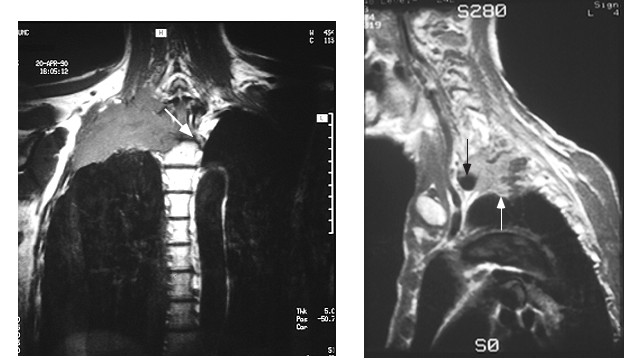
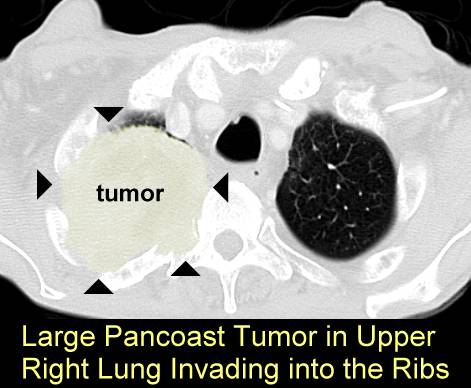
What makes Pancoast tumors unique is that the patient often presents with severe pain and neurologic symptoms but minimal lung symptoms often delaying making the correct diagnosis. CT scans and MRI scans are usually markedly abnormal (go here and here). More CT scans here, here, here
|
|
|
Pancoast Tumor seen on MRI |

The overwhelming majority of cases of Pancoast syndrome are non–small cell lung carcinoma (NSCLC), with more than 95% located in the superior sulcus, go here. The most common varieties are squamous cell carcinoma or adenocarcinoma. Small cell carcinoma is observed in fewer than 5% percent of cases in most series.
Other causes include nonepithelial neoplasms (eg, lymphoid malignancies, metastatic cancers of nonpulmonary causes), infections, lymphomatoid granulomatosis, vascular aneurysms, amyloid nodules, and cervical rib syndrome. Inflammatory pseudotumor (plasma cell granuloma), mycotic subclavian artery aneurysm, and carotid pseudoaneurysm in a child (caused by a hydatid cyst) have been reported. Because of the wide variety of diseases that can produce Pancoast syndrome, a histologic diagnosis is mandatory before initiating definitive treatment.
These patients are generaly treated with radiation and chemotherapy, sometimes followed by surgery (go here). Some good web sites: here, here, here, here, here, here
 |
|
CT scan generally shows extensive cancer but the chest Xray may show just a shadow high up in the apex of the lung |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}