Physical Principles
There are several common forms of ionizing radiation. Gamma rays and x-rays
easily penetrate body tissues and deposit their energy deep in the body.
Alpha-emitting radionuclides are hazardous only when they are inhaled,
ingested, or deposited in an open wound, because alpha particles penetrate less
than 0.1 mm in tissue. Beta particles (electrons) can penetrate to a depth
of a few centimeters.
The radiation dose of interest for assessing health effects is the dose
absorbed by specific tissues, measured in rads. The international unit of
measurement for the absorbed dose, the gray (Gy), is equal to 100 rad. Since
various forms of radiation (e.g., gamma rays and alpha particles) have
different biologic effects at the same absorbed dose, the effective dose should
be used for comparisons. The conventional unit of measurement for the
effective dose is the rem. The international unit, the sievert, is equal to 100
rem. For practical purposes, a gray and a sievert are essentially equal when
one is dealing with gamma and beta rays.
Important factors in minimizing the effects of radiation are time, distance,
and shielding. Since the absorbed dose is directly proportional to time, only
the minimal necessary amount of time should be spent in the vicinity of a
radioactive source. The absorbed dose decreases rapidly with the square of the
distance from the source. Tripling the distance from the source decreases the
dose rate to one ninth. Shielding with lead can be used as protection from
small radioactive sources. Staying indoors may be necessary for protection from
a radioactive atmospheric plume.
Radioactivity decays with time. Some radionuclides (e.g., iodines) are
short-lived, whereas others (e.g., cesium, strontium, and cobalt) have physical
half-lives of many years. The cumulative dose depends not only on the dose rate
measured at a point in time, but also on the duration of exposure and the rate
of decay. The decay rate may affect some management decisions, such as whether
to decontaminate the affected area or simply to let the radionuclide decay.
Biologic Principles
At high doses of radiation, some parenchymal cells die, but the clinical
effect may be insignificant if the cells are not critical for survival.
However, if a large number of cells are killed or if those that die are
essential for survival, clinical symptoms develop.In general, rapidly dividing
cells (e.g., intestinal-mucosa and bone marrow cells) are most vulnerable to
radiation. At doses of less than 1.0 Gy, the damage is generally not severe,
and the majority of cells survive, but they may be susceptible to subsequent
malignant transformation. In this article, we do not review the long-term
effects of radiation exposure (carcinogenesis), except to note that the
probability of radiation-induced cancer is dose-related. Leukemia can develop
as early as two years after exposure, whereas radiation-induced solid
tumors may develop after a period of 5 to 10 years or even several decades.
Types of Radiation Exposure
Radiation accidents can result in localized or whole-body exposure and in
internal or external deposition of radioactive materials (contamination). The
clinical manifestations of exposure to radiation depend on the extent of
penetration and the absorbed dose in various tissues. Recognition of acute
radiation injuries is based on the history and clinical findings.Most radiation
injuries do not constitute a medical emergency; management consists of the
treatment of symptoms and supportive care.
Localized Exposure
Localized, deep exposure to radiation is caused by direct handling of highly
radioactive sources. The patient often survives even if the absorbed doses are
very high. Because the dose rate drops rapidly as the distance from the
radioactive sources increases, systemic manifestations are not as severe as the
local injury.
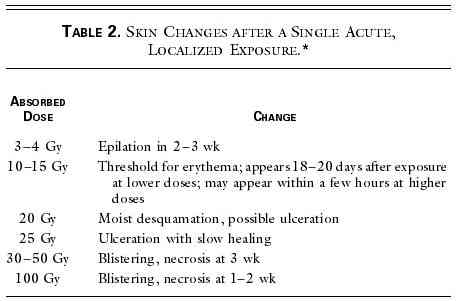
The signs of a radiation burn are similar to those of a thermal burn:
erythema and desquamation or blistering. However, the signs of a radiation burn
appear after a period of days (Table 2).
Vascular insufficiency can develop several months or years later, causing
ulceration or necrosis of tissues that had previously healed. Treatment of
localized radiation injuries usually involves prophylaxis against infection,
control of pain, and vasodilator therapy; in some cases, plastic surgery,
grafting, or amputation is required. The extent of penetration of the radiation
is an important factor in the outcome of local injury. With heavy radioactive
fallout, beta rays cause superficial skin burns, particularly on portions of
the body not covered by clothing.
Whole-Body Exposure
Abnormalities in the most susceptible tissues are manifested in the first
days and weeks after whole-body radiation exposure. A large, single exposure to
penetrating radiation can result in various forms of the acute radiation
syndrome (Table 3). Within
the first 12 hours after exposure, there is a prodromal phase, consisting of
nausea and vomiting, which lasts for up to 48 hours.
At doses exceeding 30 Gy of whole-body, penetrating radiation, cardiovascular
and central nervous system damage occurs, primarily as a result of hypotension
and cerebral edema. There is almost immediate nausea, vomiting,
prostration, hypotension, ataxia, and convulsions. Death usually occurs within
several days.
Acute, whole-body doses of approximately 10 to 30 Gy cause a gastrointestinal
syndrome, primarily as a result of the death of intestinal mucosal stem cells.
This syndrome is characterized by the rapid onset of nausea, vomiting, and
diarrhea, which is followed by a latent period of approximately one week and
then by recurrent gastrointestinal symptoms, sepsis, electrolyte imbalance,
and ultimately death.
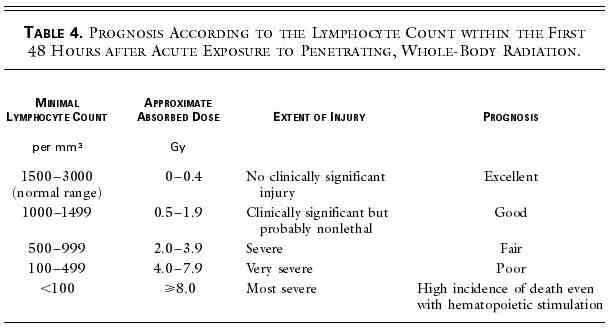
A clinically significant hematopoietic syndrome occurs after whole-body
doses of 2 Gy or higher as a result of bone marrow depression. After the
prodromal symptoms, there is a latent period of two to three weeks during which
the patient may feel well. A reduction in the lymphocyte count can occur within
48 hours after exposure, and the magnitude of the reduction is a
useful indicator of the radiation dose (Table
4). Maximal bone marrow depression with leukopenia and thrombocytopenia
occurs several weeks after exposure, when hemorrhage and infection can be
major problems. If the bone marrow is not completely eradicated, a recovery
phase ensues, which may be enhanced through use of hematopoietic growth
factors.If there is extensive skin injury, the damaged functions of the skin
may interact with other organ damage. Some authors have referred to this as
the "cutaneous syndrome."
A number of drugs that provide protection against radiation have been
suggested for use in terrorist attacks. To be effective, most of these drugs
need to be given before exposure. Amifostine is approved by the
Food and Drug Administration (FDA) for some patients undergoing radiation
therapy, but it has serious side effects, including hypotension, which severely
limit its use in emergency personnel who must engage in physically demanding
activities. Androstenediol has recently been proposed as a prophylactic drug,
but it has been evaluated only in animals. Moreover, androstenediol boosts the
immune system, which is required only if the radiation dose approaches the
lethal level. Bone marrow transplantation, which has been performed in patients
with whole-body doses in excess of 12 Gy, has not been helpful. Experience with
accidental exposure has shown that, even if the hematopoietic syndrome is
successfully treated, death invariably follows from radiation pneumonitis,
denudation of the alimentary tract, and hepatic and renal dysfunction.
Internal Contamination
Internal contamination can occur from the dispersal of powdered, liquid, or
gaseous radioactive material. The material may enter the body by inhalation or
ingestion, through intact skin, or through wounds or burns. Effective treatment
requires knowledge of both the radionuclide and the chemical form. Unless
treatment is instituted quickly, its effectiveness will be limited. There are
several general approaches to the treatment of internal contamination,
including reduction of absorption, dilution, blockage, displacement by
nonradioactive materials, mobilization as a means of elimination from tissue,
and chelation (Table 5).
In the event of the detonation of a nuclear weapon or the release of
radioactive material from a nuclear reactor, the most likely treatment of
internal contamination would be the use of potassium iodide or iodate to
prevent radioiodine from accumulating in the thyroid. The recommended daily
dose of potassium iodide is 130 mg for adults, 65 mg for children 3 to 18 years
old, 32 mg for children 1 month to up to 3 years old, and 16 mg for infants
less than 1 month old. Potassium iodide must be taken shortly before exposure
or within several hours after exposure to be effective. Both the Nuclear
Regulatory Commission and the FDA have approved the use of potassium iodide in
emergencies. Potassium iodide is widely available through the mail and the
Internet. Too high a dose will result in iodism, but the risk of serious
side effects with the recommended dose is extremely small. Chelating agents
(calcium or zinc diethylenetriamine pentaacetic acid) are investigational drugs
and are useful only if there is direct dispersal of plutonium or americium.
Such agents are not very useful for the treatment of contamination with
other radionuclides, and they are not useful after the detonation of a nuclear
weapon.
External Contamination
Radioactive contamination of clothing and exposed skin does not constitute a
medical emergency. Management of such cases of exposure is simply a matter of
removing and controlling the spread of radioactive materials. Removal
of clothing usually results in the elimination of 90 percent of the contamination.
Even extensive surface contamination is not likely to result in
overexposure on the part of medical personnel. When workers at Chernobyl who
were in the reactor area at the time of the nuclear accident were
decontaminated, the medical personnel at the site received less than 10 mGy of
radiation. Medical personnel should wear protective clothing and gloves in
conformity with universal precautions. Respirators are not required at the
hospital but should be worn by rescue personnel entering highly contaminated
areas.
If the patient has surface contamination and no physical injuries, decontamination
can be effectively performed with the use of water and detergent. If there is
substantial physical trauma, or if there are life-threatening injuries in
addition to surface contamination, the patient should be stabilized
physiologically before decontamination is performed. The skin is an important
barrier and should not be abraded during decontamination. All contaminated
materials should be placed in large, labeled plastic bags, with proper disposal
of the bags.
Contaminated Burns and Wounds
If a patient with surface contamination has a wound that is not
contaminated, it should be covered until the radioactive material has been
removed. A wound that contains radioactivity should be rinsed with saline and
treated according to conventional aseptic techniques. Excision is usually
reserved for long-lived radionuclides (especially alpha-emitting
radionuclides). If the patient has received a whole-body dose of radiation that
exceeds 1 Gy, the wound should be closed as soon as possible so that it
does not become a portal for lethal infection. Contaminated burns should be
gently rinsed and then treated in the conventional manner. Radioactive material
often comes off with the exudate or eschar.
General Management
Management of events involving the dispersal of radioactive materials can be
divided into three phases: preparation, management during the crisis, and
management of its consequences. The preparation phase includes emergency
planning, clarification of command and control issues, specification of
organizational responsibility, development of notification criteria and
communications systems, assessment of the type and quantity of equipment
required, and specification of levels of protective actions that will be taken
under certain circumstances.At all levels, the involvement of health care
facilities is crucial. Most metropolitan-area hospitals are still not
adequately prepared.
Training can be divided into training for the public and training for those
directly dealing with radiation or contamination. The specific components of
training depend on the potential level of radiation exposure and on the task at
hand. Training for emergency personnel should include information about the
nature of radiation, levels of risk, methods of protection, and
priorities for management. Training must also include mock exercises with an
emphasis on large-scale disasters and terrorist events. In addition to
training, there must be an assessment of the availability of beta–gamma
survey instruments and dose-rate meters, potassium iodide, and reference
materials. There should also be a program covering the measurement and recording
of doses, use and maintenance of dosimeters, and use of exposure information.
In the event of a terrorist incident, the Federal Bureau of Investigation is
the lead federal agency in the United States during crisis management in other
countries, an appropriate resource should be identified. Crisis management
refers to activities undertaken to ensure that there is no further threat and
to establish control over the site of the attack as a crime scene. Consequence
management refers to prevention or limitation of further damage, protection of
the public, decontamination, and disposal of radioactive material. During
consequence management, the Federal Emergency Management Agency becomes the
lead federal agency in the United States.In both phases, a federal joint operating
center is established to work with other federal agencies.
Intervention refers to actions taken to reduce the exposure to and dose of
radiation. These actions may include controlling access to the site, directing
people to stay indoors or evacuating them, removing contaminated clothing,
providing respiratory protection, administering potassium iodide, restricting
certain foods, and decontaminating property. Guidelines have been developed
that specify which actions to take if a particular dose level is likely
to be reached.
According to international recommendations, people should stay indoors for
up to two days if a dose of 1 rem is likely to be reached, with evacuation for
up to one week if the likely dose is 5 rem or higher. Temporary relocation is
recommended at a likely dose of 3 rem in the first month or 1 rem in a
subsequent month. Permanent resettlement is recommended if the lifetime dose
is expected to be 100 rem. The administration of potassium iodide is
recommended if the estimated dose to the thyroid is 100 mGy or higher. There
are similar criteria for the restriction of food and milk if the activity of
radionuclides exceeds a certain level. Experience with prior events has
provided the basis for the establishment of exposure limits and levels of radioactivity
in food and water that are thought to be safe. (Safe levels are usually defined
as those associated with a risk of death of 10–4 to 10–6
annually.)
With regard to the actions of emergency personnel, the occupational dose
limit (5 rem per year) does not apply.43 According to the
guidelines of the Environmental Protection Agency, the dose limit for
persons providing emergency services other than lifesaving activities is 5 rem
per event; for lifesaving activities, the dose can exceed 25 rem per event. The
North Atlantic Treaty Organization uses 150 rem as the limit in a disaster. The
cumulative dose is difficult to measure in emergency personnel, and dose-rate
criteria are usually used. At a dose of 0.1 mGy per hour, emergency personnel
may enter an area to perform critical, time-sensitive tasks.2
At a dose of 0.1 Gy per hour, exposure may be life-threatening, and emergency
personnel should return to their control point to await instructions from a
radiation expert on how to proceed.
Early Management
Initial management consists of on-the-scene triage and transportation of
victims to emergency rooms for treatment. The principles of handling hazardous
materials, which are based on the assumption that the toxic environment is
relatively contained, provide for maximal protection of a few workers while
they are rescuing a small number of patients. This approach will not be
practical if there are large numbers of casualties and little or no notice.
Persons with life-threatening injuries should be handled as if they were
contaminated and taken to a local hospital. Those who are uninjured or have
minor injuries should be evacuated (upwind if possible) and then evaluated for
possible contamination. The usual procedure for on-the-scene decontamination is
not adequate if there are large numbers of patients. In the event of
a chemical and biologic event, the local health care facility is primarily
responsible for decontamination, but this approach is not necessary and may
even be inadvisable in the case of widespread dispersal of radioactive
materials.
Ambulance staff should wear gowns and gloves and appropriately dispose of
the victims' outer clothing. The hospital should be informed of the imminent
arrival of seriously injured and possibly contaminated patients. Contaminated
persons who are uninjured or have only minor injuries should be taken to a
designated center for registration, decontamination (removal of clothing and
showering), and treatment of minor injuries. Persons who report nausea,
vomiting, or diarrhea should be referred to a hospital for evaluation of
whole-body exposure. If possible, the evaluation should be performed at a
facility other than the one providing care for contaminated patients who have
life-threatening traumatic injuries.
In the emergency room, patients should receive care in an area where access
is controlled (with the use of ropes and signs), and exits should be monitored
so that contamination is not spread. Security is necessary to prevent
unauthorized access. The medical staff should adopt universal precautions.
Patients can be moved with minimal spread of contamination by wrapping them in
cloth sheets. Containment of wastewater is probably not possible, and
its release can be justified in almost all situations. |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}