
Malignant Melanoma
|
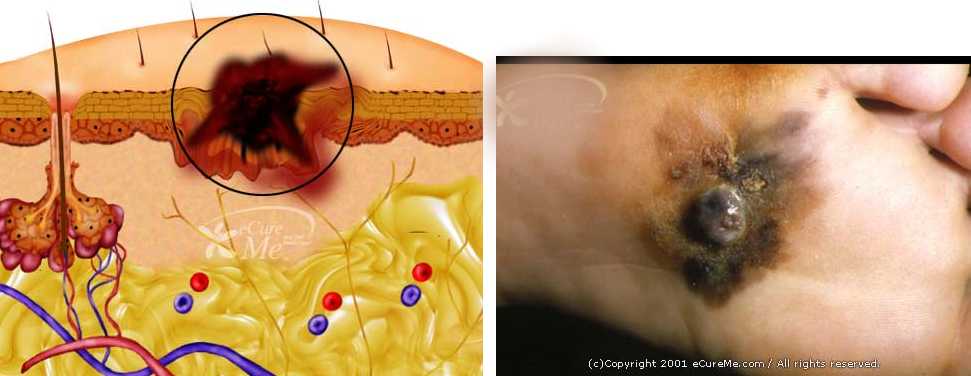
Malignant Melanoma |
the key to melanoma is early diagnosis or recognizing which moles need to be removed. See the images above, the emphasis is on the abc's of asymmetry, border, color and diameter. Treatment for melanoma is usually with surgery with radiation for spread. Chemotherapy has not been effective but studies are showing benefit from immune therapy like Ipilimumab and other targeted therapy |
|

|
All patients with advanced melanoma are encouraged to go into research trials, some of the new molecular targeted drugs are getting remarkable results as noted below |
|
|


{kind=link}
{kind=link}
{kind=link}
{kind=link}