| Bronchoalveolar cancer
is an unusual form of non-small cell lung cancer and is considered a sub-category of
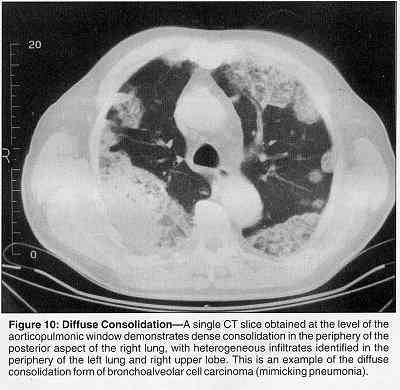
adenocarcinoma. It has the reputation of being slow growing and often multicentric
(breaking out in multiple areas of the lung.) In general it is treated similarly to
adenocarcinoma but it's management is somewhat controversial. The Bronchoalveolar subtype of adenocarcinoma accounts for up to 6% of primary lung cancers and is increasing in incidence. This subtype demonstrates a broad spectrum of radiographic findings, presenting as a solitary nodule in 43% of cases (Figure 1), multicentric or diffuse disease in 27% (Figure 2), or diffuse consolidation in 30% (Figure 3). The term "bronchoalveolar cell carcinoma" was coined by Liebow in 1960 due to controversy over the true cell of origin. The name derives from recognition of two cell types, a columnar type similar to bronchial cells and a cuboidal type reminiscent of type 2 pneumocytes. Bronchoalveolar cell carcinoma is the most histologically distinct type of adenocarcinoma, and its unique radiographic characteristics relate to its growth pattern. It uses the interior alveolar air spaces as a stroma upon which to grow. This results in the radiographic appearance of air space disease (mimicking pneumonia). Some metastatic lesions, in particular, adenocarcinoma of the pancreas, biliary tree, and colon, may produce a similar appearance when disseminated to the lungs. Like most adenocarcinomas, bronchoalveolar cell carcinoma is found in the lung periphery, and the desmoplastic response it produces will frequently give rise to a spiculated margin and a pleural tag. Bronchoalveolar cell carcinoma commonly develops in an area of lung fibrosis. The nodular form of the disease tends to be indolent, often without mediastinal involvement at diagnosis. Recurrence following surgical removal is uncommon. In contrast, the diffuse form is characterized by inexorable progression. A typical bronchoalveolar case is noted below: A 45-year-old woman with a history of cigarette smoking presented with pneumonia. A chest radiograph confirmed the presence of consolidation of the right upper lung. Her symptoms resolved with antibiotic therapy, and she had normal findings on fiberoptic bronchoscopy. Subsequent chest radiography demonstrated slowly resolving, confluent opacities in the right and left lung fields (figure 4). A high-resolution computed tomographic scan of the thorax confirmed the presence of widespread, dense consolidation in the right upper lobe, with smaller areas of peribronchovascular subsegmental consolidation throughout both lung fields. A transbronchial biopsy led to the diagnosis of bronchoalveolar-cell carcinoma. The patient died after 10 months of palliative care. The presence of nonresolving pneumonia in a smoker prompts consideration of a proximal obstructing tumor. However, several forms of non–small-cell lung cancer, including bronchoalveolar-cell carcinoma, occur more commonly in nonsmokers. Bronchoalveolar-cell carcinoma is a very uncommon variant of adenocarcinoma that is most frequently seen peripherally on chest radiographs, beyond the limits of bronchoscopic inspection, as a nodule, mass, or pneumonia-like infiltrate. It can spread through the trachea to the other hemithorax. From the NCI: Bronchoalveolar carcinoma represents 10% to 25% of adenocarcinomas and sometimes has a distinct presentation and biologic behavior. Bronchoalveolar cancer may present as a more diffuse lesion than other types of cancer; 30% to 40% of patients undergoing an attempt at surgical resection present with an infiltrate on their chest radiograph. Bronchoalveolar cancer is more common in women and in patients who do not smoke cigarettes than other histologic types of lung cancer. Alveolar cell carcinoma of the lung: a retrospective analysis of 205 patients. Harpole DH et al. Ann Thorac Surg; 46(5):502-7 1988 From 1970 to 1986, survival of 205 patients with alveolar cell carcinoma was retrospectively studied. Analysis examined the predictive value of presenting symptoms and diagnostic screening results for pathological Stage III or IV disease (advanced) and survival. The lesion presented as a peripheral mass in 121 patients (59%) and as an infiltrate in 84 (41%). Seventy-nine patients (39%) had a histological diagnosis of advanced disease by TMN staging criteria. Of the 152 deaths (74%), 117 (77%) were related to the pulmonary carcinoma. In this series, the 80 patients with Stage I disease had the best prognosis (5-year survival of 55%). There was no significant difference in disease-free survival between patients having wedge resection (N = 17) and those having lobectomy (N = 63) for Stage I disease. Recurrence
and survival following resection of bronchioloalveolar carcinoma of the lung--The Lung
Cancer Study Group experience. Bronchoalveolar carcinoma: factors affecting survival. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}