 |
Key Points
* Hodgkin's disease is a neoplastic disorder of the immune system with mounting evidence
for a lymphocytic origin of the Reed-Sternberg cell.
* Clinical presentation can include a variety of constitutional symptoms including fever,
weight loss, night sweats, and pruritus.
* The pattern of spread through the central axial lymph node system allows for curative
radiation therapy for localized disease.
* Advanced disease can be cured in more than 50% of cases by combination chemotherapy.
|
Introduction
The largely successful treatment of Hodgkins disease is one of the triumphs of
modern cancer therapeutics. The death rate in the last 30 years has decreased by two
thirds because of the introduction of effective diagnostic and therapeutic modalities. It
is fortunate that the majority of patients with the disease are young, with a median age
of 26 to 30 years. There is a bimodal distribution, with a small peak of patients aged
more than 50 years. Compared with non-Hodgkins lymphoma (41,000 new cases), Hodgkins
disease is relatively rare, with 7900 new cases estimated to have occurred in 1994. The
cause of Hodgkins disease is unknown, but the pattern of disease suggests a viral origin.
There is some resemblance to the pattern of paralytic polio because children in Third
World environments are more likely to develop the disease than are adults. The disease is
more common in the adult age groups in the temperate areas. The role of the Epstein-Barr
virus is uncertain, but genomic material of Epstein-Barr virus has been detected in at
least 50% of the tumors. There is a male predominance in the incidence of Hodgkins disease
through all age groups, with a 1.4-to-1 ratio seen in adults. Siblings of patients have an
increased (sevenfold) risk for developing Hodgkins disease. Histocompatibility antigens
associated with Hodgkins disease are A1, B5, and B18; the B18 antigen has the highest
association.
Diagnosis
The main clinical and laboratory feature of Hodgkins disease is painless
lymphadenopathy, usually confined to one or two lymph node groups. Anemia is rare, except
in advanced disease; when present, it may appear as the anemia of chronic disease, with a
microcytic pattern, a low serum iron level, and a low iron-binding capacity. Granulocytic
leukocytosis with eosinophilia may occur, usually in symptomatic patients with advanced
disease. Thrombocytopenia is unusual, except in the presence of bone marrow involvement.
Liver function studies do not predict the presence of liver involvement, but an elevated
alkaline phosphatase level is the most common abnormality of advanced liver disease.
Autoimmune phenomena are distinctly unusual, although rare instances of idiopathic
thrombocytopenic purpura, cephrotic syndrome, and hemo-lytic anemia have been reported.The
erythrocyte sedimentation rate is a nonspecific measure of disease activity and may be
markedly elevated. Approximately 30% of patients have constitutional symptoms (B
symptoms), which include fever, night sweats, and loss of 10% of body weight. Pruritus may
also be noted. Manyif not allof the constitutional symptoms are thought to be related to
the production of cytokines by the malignant cells. Clinically detected splenomegaly is
unusual and is typically a later manifestation of advancing disease. Radiographic studies
show a mediastinal mass, hilar adenopathy, or both in a high proportion of newly diagnosed
patients. Nonspecific skin changes are rare. The diagnosis of Hodgkins disease requires
the skill of an experienced pathologist or hematopathologist because the diagnosis can be
difficult to make unless the Reed-Sternberg cell is easily seen. Debate over the
immunologic lineag of the malignant cell of Hodgkins disease is controversial and this
lineage remains the subject of considerable investigation. Surface marker studies suggest
that the cell is of lymphocytic origin, but the malignant cell may be difficult to
identify in the absence of the Reed-Sternberg cell. Recent investigations suggest that the
cell of origin may be a B cell. This is especially true in the so-called
lymphocyte-predominant type. The mixed component of eosinophils, lymphocytes, plasma
cells, and fibroblasts suggests that a high percentage of the node may, in fact, not be
neoplastic. Immunoperoxidase techniques permit a panel of stains to identify the
Reed-Sternberg cell, especially by positive detection for the antigens Leu-M1 (CD15) and
Ki-1 (CD30). T he histopathologic subtypes include lymphocyte predominant (<10%,
usually with an indolent natural history), nodular sclerosis (approximately 60% to 80%),
mixed cellularity (<10%), and lymphocyte depleted (<10%). The latter two may have an
aggressive course [3,4].
Staging
Most patients present with peripheral adenopathy, with 80% or more having the
disease confined to above the diaphragm in the initial clinical assessmen Radiographic
examination of the chest, including chest roentgenography and computed tomography (CT) of
the chest and abdomen, and routine blood counts and chemistries are essential components
of this staging process [6]. Bone marrow biopsy findings are more likely to be positive in
advanced clinical disease, and biopsy is usually a routine component of staging. Gross
clinical or radiographic involvement of para-aortic or iliac nodes does not require
further abdominal staging. CT is noninvasive and is rapidly replacing lymphangiography
[5]. Unfortunately, micronodular involvement of the liver and spleen still cannot be
detected by CT. Gallium scanning is not widely used but its use is increasing, especially
in the assessment of residual masses. All staging short of laparotomy is referred to as
clinical staging. Postlaparotomy assessment is called pathologic staging. The staging
classification as recently revised (Cotswolds classification.). In addition, it is
apparent that wide field high-dose irradiation does have a higher likelihood of secondary
radiation-induced malignancy, especially lung cancer and breast cancer in adolescent
females. Recent practice has gone over to combined modality treatment, in which the fields
of radiation are reduced after regression o masses by chemotherapy.
Laparotomy
Surgical staging (laparotomy) is intended to show the presence of microscopic
involvement in abdominal lymph node sites, liver, and especially, spleen. The spleen is
the most common site of abdominal involvement. Patients who have had splenectomies have a
higher incidence of serious infections with encapsulated organisms such as Streptococcus
pneumoniae. Patients should therefore be vaccinated with polyvalent pneumococcal vaccine
or trivalent vaccine. Laparotomy is not needed unless therapy will be influenced by the
findings. An increasing body of data confirms that laparotomy per se does not influence
survival, and therefore it has been abandoned in many countries. In favorable
presentations, such as localized, asymptomatic (CS/IIA) without bulky disease, normal
sedimentation rate, and with fewer than four sites of involvement, limited radiation
(mantle field for supradiaphragmatic presentations) will suffice for three fourths of the
patients. Laparotomy staging will detect 10% to 15% abdominal involvement in favorable
patients; thus, the progression-free rate for radiation therapy only will be even higher,
in the range of 85% to 90%. The likelihood of abdominal involvement in patients presenting
with asymptomatic Hodgkins disease that is clinically confined to above the diaphragm is
30%. The incidence rises in symptomatic (B symptom) patients and is proportional to the
number of involved nodal sites. Patients with massive mediastinal tumors (more than one
third of the chest diameter) require systemic therapy and thus do not require laparotomy.
Patients with very favorable presenting features (eg, female, <26 years, with stage IA
nodular sclerosis) do not require laparotomy because the likelihood of abdominal disease
is less than 5%.In many institutions in which the policy is to offer combined-modality
therapy routinely, laparotomy may be deferred. Some of the prognostic variables associated
with an unfavorable natural history, early dissemination, or both are shown in Table 3.
Hodgkins disease is known to be associated with a defect in delayed hypersensitivity
reactivity. Advanced stages may have a marked lymphopenia. Cutaneous anergy is common but
may be reversed in patients who have achieved long-term cure. The immune defect is
attributed to suppression of normal T-lymphocyte function.. Humoral immunity is usually
intact, except in patients who have had splenectomies and combined chemotherapy and
radiation therapy.
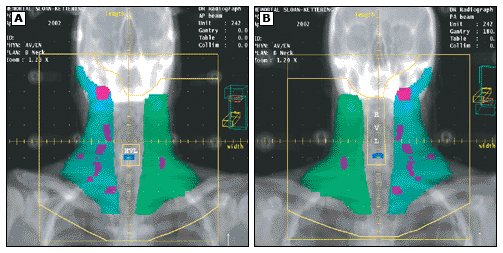
Early-Stage Disease (IA or IIA)
Disease limited to nodes on one side of the diaphragm is usually treated with
radiation therapy directed to the involved fields plus contiguous uninvolved lymph
groups. This is commonly delivered as a mantle alone or with extension over the
para-aortic area to L-2 (Fig. 1). Total nodal irradiation is rarely required for localized
disease. Primary radiation therapy alone is offered to patients who are shown to have
disease confined to stage I or II and are considered on a clinical basis to have a low
likelihood of abdominal involvement (eg, stage I disease, female, <26 years, with a
nodular sclerosis or lymphocyte-predominant subtype, or those shown to have negative
findings on staging laparotomy). The tendency is to limit the field to the mantle if the
disease is confined to the upper chest (above the carina) The long-term side effects of
radiation therapy include hypothyroidism, radiation fibrosis, effusions, and
late-occurring solid tumors in the field of irradiation. Patients who present with bulky
mediastinal masses or otherwise extensive disease, such as pericardial involvement,
require chemotherapy before radiation therapy
Advanced-Stage Disease (IIIA2, IIIB, or IV)
Radiation therapy is still an option in some patients with minimal splenic, splenic
hilar, or celiac node involvement (stage IIIA1). It is possible to effect a cure in 60% to
70% of patients with total nodal irradiation, but those with more than four gross nodules
in the spleen will require systemic therapy because of the higher rate of recurrence with
radiation therapy alone. There is a greater tendency now to offer such patients combined
modality therapy because it is associated with the lowest recurrence rate The more
advanced stages, such as IIIA2, IIIB, and IV, will require combination chemotherapy as
primary therapy, with the possibility of radiation therapy for residual masses or sites of
previous bulk disease. The role of systemic therapy has increased over the last 10 years
as data have accumulated on the superiority of combined modality therapy over radiation
therapy alone in patients with any but the most favorable prognostic features.
Combination chemotherapy
The original MOPP (mustargen, oncovin, procarbazine, and prednisone) protocol was the
pioneer regimen that demonstrated that advanced Hodgkins disease could be cured by
chemotherapy alone. Its toxic side effects included a marked myelosuppression in some
patients, and sterilizationespecially in males, but also in females aged more than 25
years. In addition, especially in conjunction with radiation therapy, the alkylating
agents contribute to a small but finite incidence of myelodysplasia or leukemia (approx
3%). The risk is higher in patients with splenectomy and in those aged more than 40 years.
A nonalkylating agentcontaining regimen previously used as a second-line protocol, ABVD,
has been shown to be equivalent (in some trials, superior) to MOPP, without the previously
mentioned toxicity. The body of data now supports the use of ABVD as the first-line
chemotherapeutic approach because it has been shown to be equivalent to all other standard
dose regimens and less toxic. Alkylating agentcontaining regimens may be used effectively
in patients who relapse from treatment with ABVD. Variations of MOPP and ABVD, including
the hybrid regimen, MOPP-ABV, have also been used. It is controversial whether hybrid
chemotherapy will be superior to ABVD. The alternation of cycles of MOPP with ABVD is
superior to MOPP used alone but not superior to ABVD alone. The major toxic effect of ABVD
is the rare serious pulmonary reaction to bleomycin. The likelihood of cure in patients
with advanced-stage disease with chemotherapy alone is 50% to 60%.Systemic therapy should
be used in almost all patients who present with clinical or pathologic evidence of stage
III and IV disease and in those who present with bulky (>one third of the diameter of
the chest) thoracic stage II disease; extensive infradiaphragmatic stage II disease; four
or more sites involved above th daphragm; or marked constitutional (B) symptoms,
especially fever and weight loss, regardless of clinical stage. The extent of radiation
therapy, if used, can be reduced to those areas of bulk disease only.
Radiation therapy
In general, radiation therapy is not added to regimens in patients who have very extensive
nodal or extranodal disease such as hepatic or bone marrow involvement. Curative therapy
is well tolerated, but a number of nonmalignant chronic toxicities may occur as long-term
medical problems. These toxicities include sterilization in males, especially after MOPP
or pelvic radiation therapy, and premature ovarian failure with early menopause in
women.Radiation therapy may result in chronic pulmonary pneumonitis and fibrosis,
especially in the presence of bleomycin, with decreased carbon monoxide diffusion and
restrictive changes. Cardiomyopathy is rare but has occasionally been noted in patients
treated with conventional doses of doxorubicin as well as in those who have received left
ventricular irradiation. Rarely, premature coronary artery disease has been noted.
Improvements in radiation technique have minimized such problem but hypothyroidism
continues to be problem following radiation treatment.
High-Dose Therapy
Lymphomas, in general, are the most drug-responsive neoplasms. Hodgkins disease in
relapse may still retain sensitivity to cytotoxic agents, especially alkylating agents.
The latter can be escalated to doses that necessitate transplantation of autologous bone
marrow or peripheral stem cells for the patient to tolerate the extent and duration of
myelosuppression. The clinical features that predict a more favorable response to
high-dose therapy are similar to those that predict a response to second-line
conventional-dose chemotherapy: good performance status, chemotherapy-sensitive relapse,
no more than two previous chemotherapeutic regimens, and absence of residual bulk disease.
The timing of high-dose therapy is still uncertain because second-line chemotherapy can
effect a high order of response in patients whose first remission lasts longer than 1
year, with 30% to 50% of patients remaining in a durable second remission at 5 years
High-dose therapy carries a potential risk for toxic death in the range of 10%, and the
immunosuppressive effect is likely to be additive; late serious infections may therefore
occur. Most trials have shown that allogeneic transplantation offers no advantage over
autologous transplantation. The toxicity of the former approach in heavily treated
immunosuppressed patients is limiting. Patients who achieve only a partial initial
remission or who relapse within 1 year represent a major challenge for salvage therapy and
could be considered for a high-dose program. Both of the major regimensCBV
(cyclophosphamide, carmustine, and etoposide) and BEAM (carmustine, etoposide, cytarabine,
and melphalan)contain carmustine, which should be used with caution in patients with
pulmonary compromise or in those who have had extensive irradiation to the chest. The
long-term (approximately 5-year) disease-free benefit from high-dose therapy is determined
by the patient mix and can vary between 20% and 40%. The introduction of hematopoietic
growth factors has shortened the duration of neutropenia. The impact of modern therapy has
been such that almost 75% of all patients who present with Hodgkins disease may be cured.
Patients should continue to be monitored for recurrence, late infections, and neoplastic
complications.. The majority of relapses occur by 3 years, but a few late recurrences will
be noted with continued follow-up. Infectious diseases should be treated aggressively
because residual impairment of immune function persists despite remission or cure of the
disease. |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}