|
|
| Metastatic melanoma to the brain: prognostic factors
after gamma knife radiosurgery. Yu C, Chen JC, Apuzzo ML, O'Day S, Giannotta SL, Weber JS, Petrovich Z .Int J Radiat Oncol Biol Phys 2002 Apr 1;52(5):1277-87 Department of Radiation Oncology, University of Southern California Keck School of Medicine, Los Angeles, CA 90033, USA. chengyu@hsc.usc.edu A total of 122 consecutive patients with 332 intracranial melanoma metastases underwent gamma knife radiosurgery over a 5-year period. Of these, 39 (32%) also received whole-brain irradiation (WBI). The median tumor volume was 0.8 cm(3) (range: 0.02-30.20 cm(3)), and the median prescribed dose was 20 Gy (range: 14-24 Gy). Median follow-up was 6.8 months. Overall median survival was 7.0 months from time of radiosurgery and 9.1 months from the onset of brain metastasis. In multivariate analysis, improved survival was noted in patients with total intracranial tumor volume <3 cm(3) (p = 0.003) and inactive systemic disease (p = 0.0065), see below, whereas other parameters studied were of lesser importance (tumor location, p = 0.056, and Karnofsky performance status, p = 0.086), or of no significance (number of lesions, WBI, age, and gender). Freedom from subsequent brain metastasis depended on intracranial tumor volume (p = 0.0018) and status of systemic disease (p = 0.034). CONCLUSIONS: Stereotactic radiosurgery is an effective treatment modality for patients with intracranial metastatic melanoma. Tumor volume and status of systemic disease are good independent predictors of survival and freedom from tumor progression. |
|
|
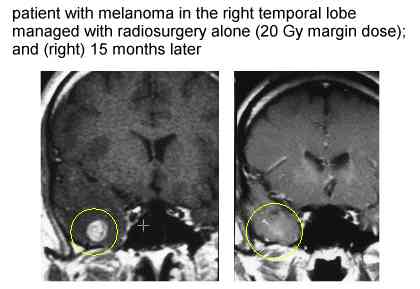
| Stereotactic radiosurgery for cerebral metastatic
melanoma: factors affecting local disease control and survival. Mori Y, Kondziolka D, Flickinger JC, Kirkwood JM, Agarwala S, Lunsford LD. Int J Radiat Oncol Biol Phys 1998 Oct 1;42(3):581-9 Department of Neurological Surgery, Center for Image-Guided Neurosurgery, University of Pittsburgh Cancer Institute, University of Pittsburgh, PA 15213, USA. The authors reviewed the management results of 60 consecutive patients with melanoma metastases, with a total of 118 melanoma brain metastases, undergoing SR during a 9-year interval. Of these, 51 also had whole-brain radiation therapy (WBRT). A total of 118 tumors of mean volume of 2.95 ml (range, 0.1-25.5 ml) were treated by SR with a mean margin dose of 16.4 Gy (range, 10 to 20 Gy). RESULTS: Median survival was 7 months after SR in all 60 patients and 10 months from brain tumor diagnosis (mean follow-up period, 9.3 months). Lack of active systemic disease and a solitary metastasis were associated with improved survival in multivariate analysis (median, 15 months). The imaging-defined local control rate of evaluable tumors (n = 72) was 90% (disappearance = 11%, shrinkage = 44%, and stable = 35%). Local recurrence developed in 7 patients and remote brain disease developed in 14 patients. WBRT combined with radiosurgery did not improve survival nor local tumor control. New brain metastases developed less often when WBRT was added to SR (23% vs. 44%), but this difference was not significant. Only 4 patients (7%) died from progression of a radiosurgery-managed tumor. No patient developed a delayed radiation-related complication, but 3 patients developed delayed intratumoral hemorrhage at the radiosurgery site, 2 of whom had new symptoms. CONCLUSIONS: Stereotactic radiosurgery for melanoma brain metastasis is effective and is associated with few complications. The use of radiosurgery alone is an appropriate management strategy for many patients with solitary tumors. see charts below |
|
|
Gamma knife radiosurgery for intracranial
metastatic melanoma: a 6-year experience. The mean survival
was 5.5 months after radiosurgery. The analyses revealed no difference in terms of
survival between patients who underwent WBRT or chemotherapy and those who did not. A
significant difference (p < 0.05) in mean survival was observed between patients
receiving immunotherapy or those with a Karnofsky Performance Scale (KPS) score of greater
than 90. CONCLUSIONS: The treatment with systemic immunotherapy and a KPS score greater than 90 were factors associated with a better prognosis.
Radiosurgery for melanoma-related brain metastases appears to be an effective treatment
associated with few complications. Gamma knife radiosurgery for malignant melanoma brain metastases. RESULTS: With a median follow-up of 75 weeks in living patients, the median survival times were 35 weeks overall: 35 weeks for patients with solitary metastases versus 33 weeks for those with multiple metastases. A factor that was significant in univariate analysis of survival was total target volume treated. This parameter remained significant on multivariate analysis. The actuarial median freedom from progression analyzed by lesion for 113 lesions in 46 patients with imaging follow-up was 89 weeks with 6-month and 1-year actuarial freedom from progression rates of 89% (95% confidence interval, 80%-95%) and 77% (95% confidence interval, 62%-87%). In univariate analysis, improved freedom from progression was associated with smaller target volume treated, smaller maximum diameter, or higher prescribed dose. Four patients (7%) developed acute Radiation Therapy Oncology Group grade > or = 2 morbidity, and five patients (9%) developed late grade > or = 2 morbidity. DISCUSSION: Median survival and freedom from progression in patients treated with radiosurgery for melanoma metastatic to the brain are comparable to results in published radiosurgery series of grouped histologies. For melanoma patients, total intracranial tumor volume appears to be of greater prognostic significance than the absolute number of metastases treated. We conclude that gamma knife radiosurgery is effective and should be considered among various management strategies. |