|
|
|
|
|
|
|
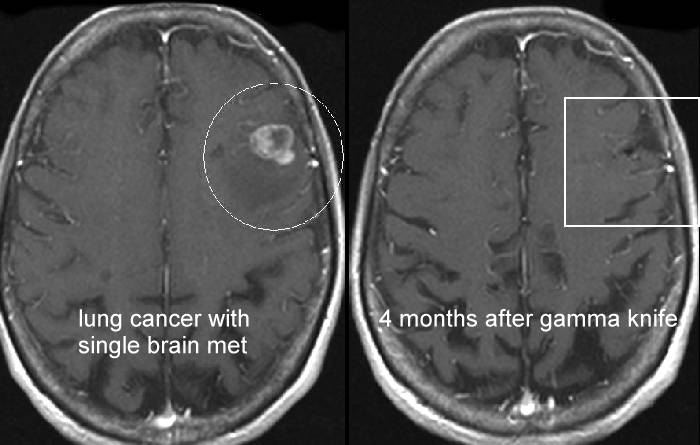
single, well circumscribed brain met, ideal for treatment with gamma knife radiosurgery |
|
|
|
|
|
|
|
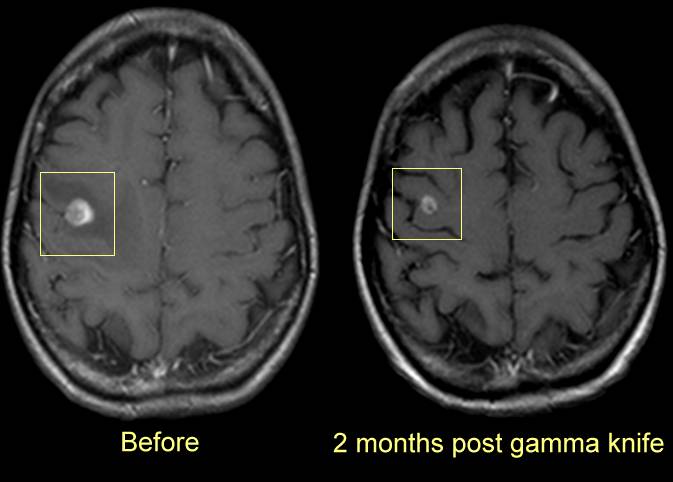
single, well circumscribed brain met, ideal for treatment with gamma knife radiosurgery |
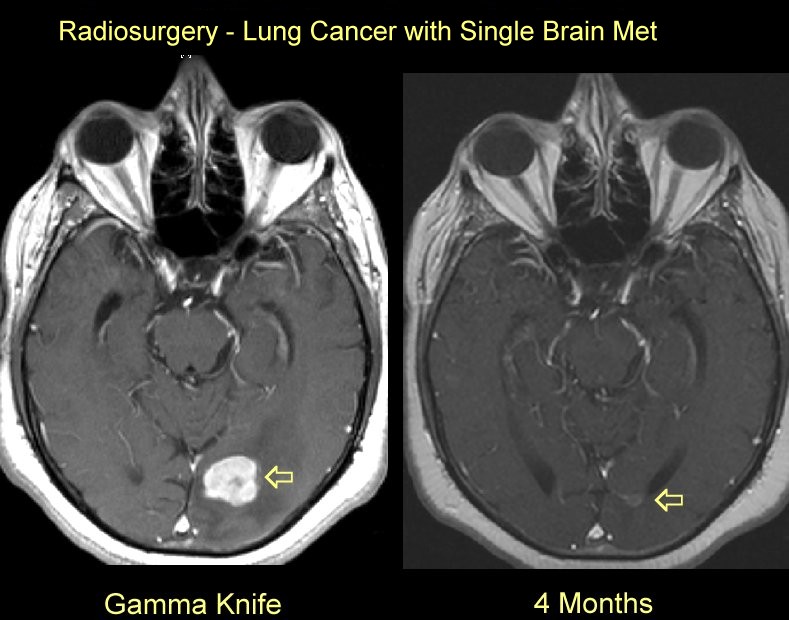
| Radiosurgery works quite well in controlling
small single brain mets (see images here
and here.) Read the review of
radiosurgery for brain metastases here. Most patients with
multiple brain metastases should probably be treated with whole brain irradiation but
selected patients can be treated with radiosurgery alone or radiosurgery combined with
whole brain radiation (see
Pitt study, German
study, U Kentucky study,
other studies,
Hopkins series, and the NCCN guidelines.) By using a
proper dose and field size, radiosurgery should control 90% of brain metastatic lesions (see studies.)
Patients who are initially treated with whole brain radiation can be
treated with radiosurgery when they relapse (see study.) Also the
RTOG study showed the patients who clearly benefit from adding radiosurgery to whole brain
radiation are those with single mets and otherwise favorable medical conditions: (see
below) the Pitt group had some long term survivors with other sites of metastases (see study.) Margins
around the tumor may extend out 1mm (see study).
In patients who have surgery to resect a met, postOp radiosurgery to the
tumor bed may be a good option and require a 2mm margin (go
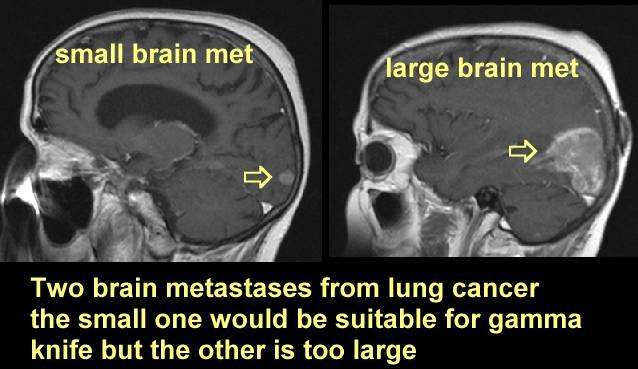
here). Size is important, radiosurgery is
best of the tumor is less than 3-4 cm (see here
and here). Location
is important, the tumor has to be moved to the center of the helmet so if the tumor is at
the edge of the brain it may be hard with a frame system to target the lesion (go here.) With the frame and helmet there are limits
if the tumor is too far lateral (x axis) the opposite side of the head or frame will
collide with the side of the helmet (referred to as a collision) if the tumor is too low
(z axis) the top of the head may collide and if the tumor is too close to the front (Y
axis) then the back of the head will collide. Frameless radiosurgery techniques do not
have this limitation. |
| Group | Radiosurgery + Whole Brain XRT | Whole Brain XRT |
| Solitary Brain Met | 6.5 months | 4.9 months |
| RPA Class I | 11.6 months | 9.6 months |
| Age < 50y | 9.9 months | 8.3 months |
| NSCL or Squamous | 5.9 months | 3.9 months |
| KS 90-100 | 10.2 months | 7.4 months |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}