The Gamma Knife procedure has been proven highly effective in the
treatment of certain malignant and benign brain tumors, arteriovenous malformations and
trigeminal neuralgia. In addition, treatments for Parkinson's disease, epilepsy, and
intractable pain are showing promising research results. The Gamma Knife treats the
patient with 201 individual gamma rays, targeted with great precision to converge on small, well circumscribed
and critically located structures in the brain.
Stereotactic radiosurgery is defined as the delivery of a single, high dose of radiation
through the intact skull to a small and critically located intracranial volume. The gamma
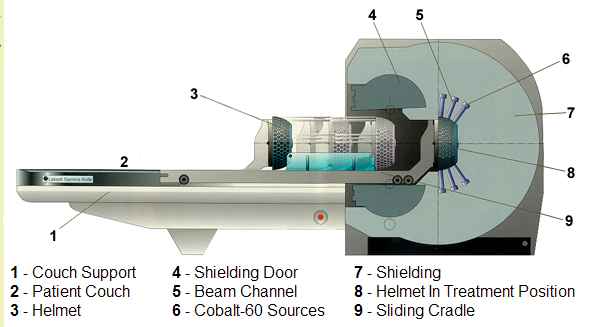
knife contains 201 cobalt-60 sources of approximately 30 Curies each at the time of
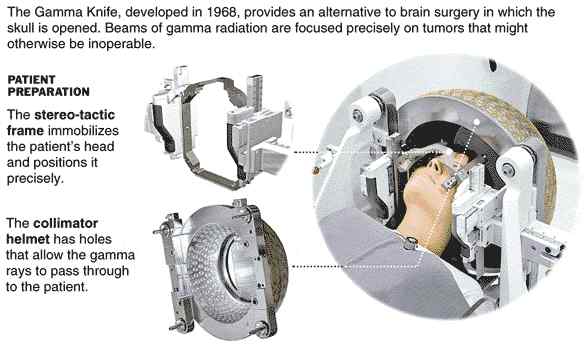
loading, placed in a hemispherical array in a heavily shielded unit. A collimator helmet
focuses the radiation to a specific target point within the head with sub-millimeter
positioning accuracy in such a fashion that a high dose of radiation is delivered to the
target while sparing the surrounding tissue. Complex-shaped lesions are treated by
combining collimators of different sizes with selected beam blocking and weighting using a
sophisticated computer planning system. This ensures that tight conformation of the dose
to the edge of the target volume is achieved such that each patient receives a
"tailored" plan. Unlike the linear accelerator, the gamma knife has few moving
parts thereby eliminating many sources of inaccuracy and unreliability. Because the
radiation fall off is very steep outside the target area, the surrounding brain receives
little radiation thereby minimizing harmful side effects to neighboring critical
structures.
Long-term results after radiosurgery for benign intracranial tumors.
Kondziolka D, Nathoo N, Flickinger JC, Niranjan A, Maitz AH, Lunsford LD.
Neurosurgery. 2003 Oct;53(4):815-21;
Departments of Neurological Surgery and Radiation Oncology, University of Pittsburgh
School of Medicine, Pittsburgh, Pennsylvania, USA. kondziolkads@msx.upmc.edu
We evaluated 285 consecutive patients who underwent radiosurgery for benign intracranial
tumors between 1987 and 1992. Our series included 157 patients with vestibular
schwannomas, 85 patients with meningiomas, 28 patients with pituitary adenomas, 10
patients with other cranial nerve schwannomas, and 5 patients with craniopharyngiomas.
Prior surgical resection had been performed in 44% of these patients, and prior
radiotherapy had been administered in 5%. The median follow-up period was 10 years.
RESULTS: Overall, 95% of the 285 patients in this series had
imaging-defined local tumor control (63% had tumor regression, and 32% had no
further tumor growth). The actuarial tumor control rate at 15 years was 93.7%. In 5% of
the patients, delayed tumor growth was identified. Resection was performed after
radiosurgery in 13 patients (5%). No patient developed a radiation-induced tumor.
Eighty-one percent of the patients were still alive at the time of this analysis. Normal facial nerve function was maintained in 95% of patients
who had normal function before undergoing treatment for acoustic neuromas. CONCLUSION:
Stereotactic radiosurgery provided high rates of tumor growth control, often with tumor
regression, and low morbidity rates in patients with benign intracranial tumors when
evaluated over the long term. This study supports radiosurgery as a reliable alternative
to surgical resection for selected patients with benign intracranial tumors.
Oncology (Huntingt) 1998 Aug;12(8):1181-8, 1191;
discussion 1191-2
Clinical uses of radiosurgery.
Chang SD, Adler JR Jr, Hancock SL
Department of Neurosurgery, Stanford University
School of Medicine, Stanford, California, USA.
Radiosurgery uses stereotactic targeting methods
to precisely deliver highly focused, large doses of radiation to small intracranial tumors
and arteriovenous malformations (AVMs). This article reviews the most common clinical
applications of radiosurgery and the clinical results reported from a number of series
using either a cobalt-60 gamma knife or linear accelerator as radiation sources. Radiosurgery is used to treat malignant tumors, such as selected cases of
brain metastases and malignant gliomas (for which stereotactic radiosurgical boosts are
utilized in conjunction with fractionated radiation therapy), as well as benign tumors,
such as meningiomas, acoustic neuromas, and pituitary adenomas. Treatment of small AVMs is
also highly effective. Although radiosurgery has the potential to produce complications,
the majority of patients experience clinical improvement with less morbidity than occurs
with surgical resection. |


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}