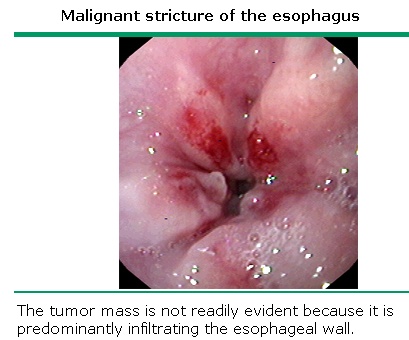
Diagnosis and staging of esophageal cancer INTRODUCTION — Squamous cell carcinoma and adenocarcinoma account for more than 95 percent of esophageal malignant tumors. For most of the twentieth century, squamous cell carcinomas comprised the vast majority of esophageal cancers. In the 1960s, squamous cell cancers accounted for more than 90 percent of all esophageal tumors in the United States, whereas esophageal adenocarcinomas were considered so uncommon that some authorities questioned their existence. For the past two decades, however, the incidence of adenocarcinoma of the esophagus has increased dramatically in Western countries so that the two tumors now occur with almost equal frequency The two forms of esophageal cancer differ in a number of features, including the location of the tumor and predisposing factors (show table 1). Smoking and alcohol are major predisposing factors for squamous cell tumors while Barrett's esophagus with specialized intestinal metaplasia (a complication of gastroesophageal reflux disease [GERD]) and possibly GERD itself are the only known major risk factors for adenocarcinoma. Survival statistics for the symptomatic patient with esophageal cancer are poor and very highly correlated with staging. The diagnosis and staging of esophageal cancer with emphasis upon endoscopic techniques will be reviewed here. The epidemiology, clinical manifestations, and the role of largely palliative endoscopic techniques in the treatment of esophageal cancer are discussed separately. DIAGNOSTIC TESTING — Although barium studies may suggest the presence of esophageal cancer, the diagnosis is usually established by endoscopy. Early esophageal cancer may appear as a superficial plaque or ulceration (show endoscopy 1). Advanced lesions may appear as a stricture (show endoscopy 2), an ulcerated mass (show endoscopy 3), a circumferential mass (show endoscopy 4), or a large ulceration. Biopsy — The endoscopic appearance of a large mucosal mass is frequently diagnostic of esophageal cancer. Biopsies confirm the diagnosis in more than 90 percent of cases Early studies found that the greater the number of biopsies taken (up to seven), the higher the accuracy. As an example, in a series of 202 consecutive patients, 47 of whom had gastric or esophageal carcinoma, the percentage of correct diagnoses of esophageal carcinoma were as follows
The addition of brush cytology specimens to seven biopsies increased the accuracy to 100 percent. Seventeen percent of lesions thought to be benign endoscopically were subsequently proven to be malignant. In vivo staining — In vivo staining of the esophageal mucosa (chromoendoscopy) can help direct the area of biopsy and determine the extent of disease. Lugol's iodide reacts with the glycogen components of normal squamous mucosa to produce a greenish brown color, while neoplastic tissue is depleted of glycogen and remains unstained. Its role in the diagnosis and screening esophageal cancer has not been established, although limited data suggest that it can be helpful in some high-risk settings STAGING — The outcome of esophageal cancer is strongly associated with its stage. As a result, accurate clinical staging is critical for selecting an appropriate treatment option. Staging usually begins with a CT scan to evaluate for the presence of metastatic disease. Patients without evidence of metastatic disease by CT frequently undergo endoscopic ultrasonography (EUS), which uses a high frequency ultrasound transducer to provide detailed images of esophageal masses and their relationship with the five-layered structure of the esophageal wall. Miniature ultrasound probes that are placed through the accessory channel of an endoscope with high ultrasound frequencies (typically 20 mHz) have also been used to accurately stage mucosal malignancies. EUS provides the most accurate estimate of disease stage and assists with management decisions. The accuracy of EUS staging has been investigated in a large number of patients and sites using operative specimens. EUS consistently provides better regional TNM tumor staging than CT scanning. Local invasion of the middle esophagus is well documented by CT, but CT is much less accurate for detecting lymph node metastases. One advantage of CT is that it detects distant solid organ metastases with an accuracy of over 90 percent. However, EUS may be less accurate for staging patients who have undergone preoperative chemoradiotherapy. In one report, for example, EUS correctly predicted a complete response to chemoradiotherapy in only 3 of 17 patients (17 percent) who had no residual tumor demonstrated in resection specimens [9]. This study suggests that different criteria will be needed to predict regional malignancy. Measuring the change in maximal cross-sectional area pre- and post-chemoradiotherapy may be a more useful measure to assess the response of esophageal cancer to preoperative chemoradiation The TNM staging system of the American Joint Committee on Cancer (AJCC) and the International Union Against Cancer (UICC) for esophageal cancer is used universally. The importance of staging is reflected in prognosis. Reported five-year survival rates for stages I to IV disease are 60, 31, 20, and 4 percent, respectively T1 esophageal tumors — Early esophageal cancer is usually diagnosed endoscopically by recognizing small mucosal defects or nodules. T1 masses are those tumors that are localized to either the mucosa or lamina propria (T1a) or submucosa (T1b) by EUS. T1 lesions are usually seen with EUS and are staged as such by determining that the mass does not involve the muscularis propria. With traditional endoscopic ultrasound using transducers with a frequency of less than 12 mHz, it may be difficult to identify and stage a mucosal malignancy. High frequency ultrasound probes can accurately stage early lesions and help determine which ones can be treated with local excision alone (T1a tumors). T2, T3, and T4 esophageal tumors — T2, T3, and T4 tumors are readily seen on endoscopy, and appear as either a stricture, ulceration, or an exophytic mass
The presence of an irregular outer border suggests that a mass has invaded through the wall of the esophagus. In addition, measurement of maximal thickness of the esophageal mass can also predict extraesophageal extension. In one report, for example, T3-T4 masses had a significantly greater thickness than T1-T2 masses (16 versus 8.2 mm). The thickness of the tumor was a more accurate predictor of staging (which was determined by esophageal resection) than muscularis disruption. A caveat for EUS staging of esophageal lymph nodes is that the instrument cannot traverse a tumor-induced stenosis (which occurs in about 30 percent of cases). In these settings, EUS may understage the tumor, since the entire lesion and the celiac axis are not seen. It is controversial as to whether to dilate the esophagus for the purpose of a staging examination, since perforations have occurred. An alternative is to use miniature EUS probes, which are passed through the biopsy channel of an endoscope. However, these devices only provide a partial solution to the problem because of the limited depth of penetration (approximately 3 cm). A nonoptical, wire-guided echoendoscope is another alternative that allows for complete EUS staging in the majority of patients Regional lymph nodes — EUS can provide nodal staging of esophageal cancer by either imaging nodes in detail or guiding needle biopsies. Malignant lymph nodes appear as large (>1 cm), rounded, hypoechoic structures with a discrete border often directly adjacent to an esophageal mass. EUS has an accuracy of more than 80 percent for detecting metastatic nodes in the cervical paraesophageal, right recurrent laryngeal, left paratracheal, upper and lower paraesophageal, infraaortic, infracarinal, and lower posterior mediastinal regions Its sensitivity is highest for cervical and upper thoracic paraesophageal, infracarinal, left paratracheal, and recurrent laryngeal nodes. Accuracy is maximum for periesophageal nodes and varies inversely with the axial distance of the nodes from the esophageal axis. The accuracy is further increased when nodes are aspirated, but this can only be performed in nodes that are accessible and in which the primary tumor is not in the pathway of the aspiration needle. The most important nodal group to be examined is the celiac area. The finding of a malignant node in the retrogastric area remote from the primary tumor is a sign of unresectability or distant metastatic disease. Several approaches are being evaluated in an attempt to improve the accuracy of regional lymph node staging for esophageal cancer. Thoracoscopic and laparoscopic staging accurately assess thoracic and celiac node status. In one multiinstitutional study conducted by the Cancer and Leukemia Group B, for example, noninvasive testing methods (CT, MRI, EUS) were found to each incorrectly identify disease status (either falsely negative lymph nodes or the presence of metastatic disease) in 50, 40, and 30 percent of patients, respectively, as assessed by thoracoscopic or laparoscopic staging Similar results were noted in another report of 26 patients, in which laparoscopy and thoracoscopy appeared to be more accurate than EUS. EUS suggested NO disease in eight patients, while laparoscopy and thoracoscopy documented N1 disease in six of the eight. Laparoscopy and thoracoscopy also had the advantage of allowing evaluation of the thoracic and abdominal cavities for metastases. Immunohistochemical examination of lymph nodes is another method that may significantly improve pathologic staging. In a study of 1308 lymph nodes from 68 patients with esophageal cancer without overt metastases who underwent radical en bloc esophagectomy, 399 were found to be free of tumor by routine histopathology. These nodes were further studied by immunohistochemistry with the monoclonal antiepithelial-cell antibody Ber-EP4; 67 (17 percent) stained positively. Fifteen of 30 patients considered free of lymph node metastases had such cells in their lymph nodes. The finding of positive staining in nodes thought to be metastasis-free had predictive prognostic significance; positive cells predicted relapse in both patients without nodal metastases and in those with regional lymph node involvement. All 12 patients whose lymph nodes were negative on both histopathologic and immunohistochemical analysis survived without recurrence. Distant metastases — M staging has been primarily performed using CT scanning. While relatively inexpensive, CT is limited in its ability to identify locally advanced or subclinical metastatic disease, particularly in the peritoneal cavity. EUS is being increasingly used for this purpose since it can diagnose liver metastases <1 cm or malignant ascites; needle aspiration can provide a tissue diagnosis for either of these findings. Other staging modalities, laparoscopy and PET scanning, have been used to improve the detection of patients with occult metastases, in an attempt to limit aggressive treatment to those who are most likely to benefit from it. In at least one study of 26 patients with gastric or esophageal cancer, M staging accuracies for laparoscopic US versus laparoscopy versus CT were 89, 44, and 64 percent respectively . However, laparoscopy is invasive, and requires hospitalization and general anesthesia. PET scans — Positron emission tomography (PET) with 18F-fluorodeoxyglucose is a noninvasive staging modality that is more sensitive than CT for the detection of distant metastases]. In two studies totaling 94 patients, PET prevented needless surgery in 22 who had metastatic disease undetected by CT aloneIn a study of 91 patients with esophageal cancer, PET scans detected 51 metastases in 27 of 39 cases (69 percent sensitivity, 93.4 percent specificity, 84 percent accuracy) and was more accurate than CT at detecting distant metastases In contrast to improved detection of metastatic disease, PET scans are not as useful in the evaluation of the primary site and locoregional nodes. One study prospectively compared PET scanning to preoperative CT and EUS in 74 patients with potentially operable cancer of the esophagus or GE junction. At the primary site, PET scanning showed increased activity in 70 of 74 patients, but was falsely negative in four patients with T1 tumors. Thirty of the 74 patients underwent lymphadenectomy at the time of esophageal resection. PET scanning was not as sensitive as EUS for the detection of local lymph nodes (sensitivity 33 versus 81 percent) and had only slightly better specificity (89 versus 67 percent). Nevertheless, the improved sensitivity of PET for the detection of metastatic disease makes it potentially the most cost-effective method of identifying patients with occult metastases, for whom aggressive therapy should not be pursued. This hypothesis was directly tested in a decision analysis model that compared several different staging strategies, and was conducted in parallel with a prospective clinical trial. When compared with the staging strategy of CT plus EUS/FNA, PET plus EUS/FNA was slightly more expensive (by $4158 on average), and only associated with a one-month benefit in quality adjusted life years. The marginal cost-effectiveness ratio of this strategy ($60,544 per QALY) did not compare favorably with other accepted medical treatments. The use of PET scanning for initial staging of esophageal cancer is covered by Medicare. Preoperative bronchoscopy with biopsy and brush cytology has been advocated by some as the last investigation in the staging workup, and is reasonable in patients with advanced tumors of the proximal esophagus. In one study of 116 consecutive patients with potentially operable esophageal carcinoma, bronchoscopy was superior to CT and was the sole decisive procedure resulting in exclusion from surgery because of airway invasion in 10 percent of patients SUMMARY AND RECOMMENDATIONS — The diagnosis of esophageal cancer is usually established by endoscopy Early esophageal cancer may appear as a superficial plaque or ulceration). Advanced lesions may appear as a stricture , an ulcerated mass a circumferential mass , or a large ulceration. The endoscopic appearance of a large mucosal mass is frequently diagnostic of esophageal cancer. Biopsies confirm the diagnosis in more than 90 percent of cases Staging usually begins with a CT scan to evaluate for the presence of metastatic disease. Patients without evidence of metastatic disease by CT frequently undergo endoscopic ultrasonography (EUS), which uses a high frequency ultrasound transducer to provide detailed images of esophageal masses and their relationship with the five-layered structure of the esophageal wall. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}