| Current Application and Research Directions for
Partial-Breast Irradiation Oncology April 2007 • Volume 21 Number 4 Prior to the 1970s, the treatment of breast cancer was dominated by radical mastectomy or modified radical mastectomy of the affected breast . This consists of an en bloc removal of the breast, muscles of the chest wall, and contents of the axilla and was advocated as the most appropriate local therapy for women with early-stage breast cancers. However, the results of the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-06 trial and other studies, found equivalent survival and local control rates among women treated with breast-conservation therapy (BCT)—either mastectomy or lumpectomy followed by whole-breast irradiation (WBI). The NSABP B-06 trial, which compared mastectomy to lumpectomy with and without radiotherapy in women with invasive carcinoma, found a 39% local recurrence rate at 20 years with lumpectomy alone, which was decreased to 14% with the addition of radiotherapy. Several other randomized studies demonstrated equivalent long-term survival and disease-free survival rates in patients treated by BCT compared to mastectomy. Additional randomized studies comparing lumpectomy alone to lumpectomy and radiation clearly demonstrate a threefold reduction in local relapse with the use of radiation following breast-conserving surgery. More recent meta-analysis of trials comparing lumpectomy alone to lumpectomy and radiation demonstrated not only a threefold higher local relapse rate with the omission of radiation following lumpectomy, but also a small yet statistically significant compromise in overall survival. For patients with ductal carcinoma in situ (DCIS), randomized studies comparing lumpectomy alone to lumpectomy plus radiation, conducted by the NSABP and European Organisation for Research and Treatment of Cancer (EORTC), found a 55% and 43% reduction in ipsilateral breast cancer events, respectively, with the addition of radiotherapy. As a result of these data, breast-conservation surgery followed by whole-breast irradiation (BCS+RT) became the standard of care for women with stage 0, I, and II breast cancer. BCS+RT involves the surgical removal of the primary tumor, evaluation of the axillary nodes, followed by whole-breast irradiation. This treatment is extremely well tolerated with minimal long-term complications and favorable cosmetic outcomes. Despite the obvious cosmetic and potential psychosocial advantages of BCS+RT, 15% to 30% of patients who undergo lumpectomy do not receive postoperative radiotherapy. Many patients may choose mastectomy or lumpectomy alone over BCS+RT due to the protracted course of daily treatment involved with WBI, which consists of daily radiotherapy to the whole breast for 25 treatments usually followed by a boost to the tumor bed, delivered over the course of 6 to 6.5 weeks. Other reasons that may steer women away from BCS+RT have been identified as physician bias, patient age, fear of radiation treatments, distance from a radiation treatment facility, and socioeconomic factors. Search for an Alternative to WBI Based on the numerous randomized studies noted above, it is standard of care for all women, regardless of age or tumor size, to receive radiotherapy in the setting of BCT to reduce local recurrence. However, in recent years, investigators have tried to identify subsets of women who may not benefit from the addition of radiotherapy to lumpectomy for early-stage breast cancer. A prospective study from the Cancer and Leukemia Group B (CALGB) randomized women 70 years of age or older with tumors that were estrogen-receptor-positive and less than 2 cm in diameter to tamoxifen with or without radiotherapy. In this randomized trial, even though radiotherapy significantly reduced the rate of local recurrence (from 4% to 1%), there was no difference in overall survival, and the investigators concluded that "tamoxifen alone is a reasonable choice for adjuvant treatment in such women." Published simultaneously, a Canadian trial in women over age 50 with early-stage breast cancer demonstrated a local relapse rate of 7.7% with lumpectomy and tamoxifen compared to 0.6% with lumpectomy, tamoxifen, and radiation. Although there was no compromise in survival with the omission of radiation in either trial, these studies were not powered sufficiently to detect small benefits in survival. Smith et al, using the Surveillance, Epidemiology, and End Results (SEER)-Medicare database, identified 8,724 women over age 70 years who met the eligibility criteria for CALGB 9343. They compared those women over age 70 treated with radiotherapy following lumpectomy to those treated by lumpectomy alone. In this nonrandomized study, they found that radiotherapy not only reduced local recurrence but also reduced the rate of any second breast cancer event and subsequent mastectomy. They further identified subgroups, such as women between 70 and 79 years with low comorbidities and those with lobular histology, who derived the greatest benefit from radiotherapy. Of note, in the SEER-Medicare database of women age 70 or greater, only 59% of patients treated with breast-conserving surgery received radiation. Collectively, these data suggest that for older women, although radiation may be safely avoided, it is rational for elderly women with long life expectancies and low comorbidities to receive radiotherapy after lumpectomy, given its benefit. However, many fail to do so in light of the prolonged course of therapy, resources involved in travel, and distance to a radiotherapy center. Introduction of APBI In response, accelerated partial-breast irradiation (APBI) has been studied increasingly over the past 15 years as a viable alternative to WBI. In general, APBI involves treating the surgical cavity with a 1- to 2-cm margin, thus reducing the volume of irradiated breast tissue by up to 50% using various radiotherapeutic methods. Technical approaches of partial-breast irradiation include multicatheter interstitial brachytherapy, balloon catheter brachytherapy, three-dimensional conformal external-beam radiotherapy (3D-CRT) and intraoperative radiotherapy (IORT). Treatment is typically delivered postoperatively, over a short period of time, using large fraction sizes. Advocates of APBI state that it is a safe, well tolerated therapy that allows for equivalent cosmetic outcomes while significantly increasing quality of life and allowing for an effective treatment of the patient's breast cancer. To date, pilot studies of various APBI techniques have been studied, and large, multicenter, randomized controlled studies are underway comparing APBI to WBI. Rationale In standard BCS+RT, radiotherapy is delivered to the whole breast to eliminate areas of occult multicentric in situ or invasive carcinoma. Additional radiotherapy may be delivered to the tumor bed using a boost to eliminate the higher burden of microscopic disease that may have been left in close proximity to the tumor bed after lumpectomy. Following BCS and whole-breast irradiation, the majority of local relapses occur in close proximity to the tumor bed. When discussing a tumor recurrence in the ipsilateral breast, it is important to note the difference between a true recurrence and the development of a second primary in the irradiated breast. A study from Yale described the development of a new primary when the recurrence was distinctly different from the primary tumor with respect to the histologic subtype, location, or ploidy. In their studies of patients treated with BCT with 15 year data, patients developed both true recurrences and new primaries at similar rates until approximately 8 years, when true recurrence rates stabilized but new primary rates continued to rise. Recht et al also found that the majority of true recurrences occurred in the first 5 to 10 years, but with increasing follow-up, they saw a higher incidence of second primary tumors that developed in other quadrants of the breast. The 20-year update from Veronesi et al comparing mastectomy to BCT showed a nonsignificant difference between the development of new primaries in the ipsilateral breast (0.42 per 100 woman-years of observation) treated with BCT compared with the contralateral breast (0.63 per 100 woman-years of observation). Several retrospective as well as prospective studies evaluating patterns of local relapse following BCS with or without radiation have shown that the majority of tumor recurrences occurred at or near the original tumor bed. Veronesi et al found that failures beyond the lumpectomy cavity occurred in 2.9% of patients, consistent with previously published data of 1.5% and 3.5%, These data suggest that the true benefit to radiotherapy may be to decrease the recurrence of tumor at or near the tumor bed, but may not prevent the development of new, second primary breast cancers that may occur elsewhere in the irradiated breast. Anatomic data on the distribution of tumor cells in relation to the primary lesion have been published in surgical series. Holland et al reviewed 217 mastectomy specimens from patients in the Netherlands with tumors less than 4 cm. They reported that the presence of an extensive intraductal component (EIC) was associated with a substantial likelihood of having residual disease located beyond a 2-cm margin from the primary tumor, whereas in patients without an EIC, it was rare for cancer foci to be found more than 2 cm from the primary tumor. In a recent abstract presented at the European Society for Therapeutic Radiation Oncology (ESTRO) meeting in 2006, Holland studied pathologic and mammographic criteria to identify breast carcinomas of limited extent, defined as an absence of microcalcifications or tumor density beyond the edge of the primary lesion based on mammography and a 1-cm tumor-free margin out of a 2-cm gross surgical margin based on pathology. The group found that 89% of patients who met these criteria were correctly identified as having a true breast carcinoma of limited extent. The authors concluded that by carefully examining radiographic and pathologic data, one may be able to correctly identify patients who may be candidates for "surgical excision of the tumor followed by partial-breast irradiation." The fact that a majority of true local relapses occur in close proximity to the tumor bed, along with available pathologic data demonstrating minimal microscopic tumor burden more than 1 to 2 cm beyond the primary tumor, provides a rationale for more localized treatment in selected patients. With APBI, a conformal dose of radiation is delivered to a limited volume of breast in a short period of time. Unfortunately, the majority of data regarding APBI involves single-institution, nonrandomized studies with small patient populations. While these data are promising, it is clear that to firmly establish APBI as an acceptable alternative to WBI, prospective randomized studies are necessary. Recently, an intergroup trial (NSABP/Radiation Therapy Oncology Group [RTOG]) launched a large randomized study comparing WBI to APBI for women with early-stage invasive and noninvasive breast cancer. Accrual has been brisk and is expected to close earlier than expected. Patient Selection Accurate patient selection for APBI is critical to prevent locoregional failures. To date, the American Brachytherapy Society (ABS) and the American Society of Breast Surgeons (ASBS) have released similar versions of patient selection criteria for APBI, based mainly on single-institution, retrospective and prospective studies (Table 1).
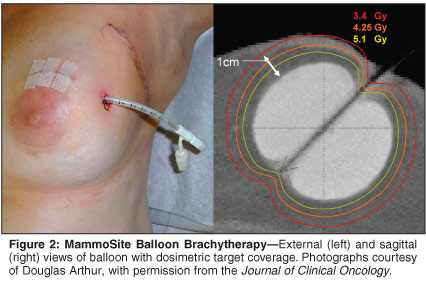
The ABS criteria for patient selection include age older than 45 years, tumor ≤ 3 cm in greatest dimension, invasive ductal histology, negative lymph node status, negative marginal status (defined as "no tumor at ink"), applicator placement within 10 weeks of final lumpectomy procedure, and a postlumpectomy cavity with one dimension of at least 3.0 cm. Very similar to the ABS recommendations, the ASBS recommendations include age older than 45 years, tumor ≤ 3 cm in greatest dimension, in situ or invasive ductal histology, negative lymph node status, and negative marginal status (defined as 2 mm in all directions). However, the criteria developed by these societies are based on data from small, nonrandomized studies from single-institution experiences. Prospective, randomized studies are needed to further elucidate patients that may or may not benefit from APBI. The NSABP B-39/RTOG 0413 trial randomizing patients to WBI vs APBI uses the following criteria: age ≥ 18 years, in situ or invasive ductal histology, tumor size ≤ 3 cm, negative margins, a target lumpectomy cavity ≤ 30% of the breast volume, and, if invasive histology, 0 to 3 positive axillary nodes with a minimum of 6 sampled nodes, or negative sentinel node. This study will help to further refine selection criteria for APBI, including whether patients in younger age groups, patients with ductal carcinoma in situ, and patients with limited positive nodal status are suitable candidates. Given the survival benefit seen in patients with positive nodes after mastectomy and irradiation of the chest wall and regional nodal groups, inclusion of patients with positive nodes as candidates for APBI without regional nodal irradiation has been debated. Other clinicopathologic features such as extensive intraductal component, invasive lobular histology, and lymphovascular invasion still need to be investigated. The results of the NSABP/RTOG randomized trial, which includes patients with these features, may help to refine selection criteria for women considering APBI as an alternative to WBI. Until more data are available, it appears that the use of APBI per ABS or ASBS recommendations represents a reasonable cohort of patients to consider for partial-breast irradiation. However, we advise the enrollment of patients for APBI on clinical trials, to help to identify selection criteria, document patterns of recurrence as well as acute and long-term toxicities, and develop alternative technical approaches and fractionation strategies. Current Techniques and Experience in APBI The goal in APBI is to deliver a homogeneous dose of radiation in a short period of time to the tumor bed with additional margin. This may be achieved using several distinct radiotherapy techniques and include multicatheter interstitial brachytherapy, balloon catheter brachytherapy, 3D-CRT, and intraoperative radiotherapy (IORT), each of which is vastly different from one another in terms of degree of invasiveness, radiation delivery, operator proficiency, acceptance among radiation oncologists, and length of treatment. These techniques are able to deliver a homogeneous dose of radiation to the target area, which in theory is radiobiologically equivalent to conventional protracted whole-breast irradiation with respect to local tumor control, and acute and long-term toxicity. A considerable amount of phase I/II data are available from investigations of APBI, with local control rates similar to those of WBI at 5 years. However, most of these data evolved from patients who received multicatheter interstitial breast brachytherapy, which is an intricate, labor-intensive procedure that requires skill on the part of the radiation oncologist. More recently, the MammoSite balloon catheter, external-beam radiotherapy (EBRT), and intraoperative radiotherapy have been investigated as alternative methods of APBI. MammoSite Balloon Catheter Brachytherapy The MammoSite balloon brachytherapy device (MammoSite Radiation Therapy System; Cytyc Corp; Marlboro, Mass), introduced in 2002, is a form of intracavitary brachytherapy that is simpler than interstitial brachytherapy in terms of technique and treatment planning. The apparatus consists of a double-lumen catheter that is 15 cm in length and 6 mm in diameter. The catheter contains a central lumen that allows for a high-dose-rate Ir-192 source, while the balloon is located distally. The balloon is available in two sizes when inflated—either 4-5 cm or 5-6 cm in diameter—for variability in the dimensions of a lumpectomy cavity. The catheter is implanted after lumpectomy either at the time of surgery directly into the cavity, after surgery under ultrasound guidance through a small, separate incision, or after surgery directly into the cavity through the healing lumpectomy wound. After catheter placement, computed tomography (CT) of the breast is performed prior to initiation of treatment to determine whether the balloon-to-skin distance is ≥ 5 mm, the conformity of the balloon to the walls of the lumpectomy cavity is > 90%, and symmetry exists between the balloon and the center shaft of the catheter (Figure 2). These guidelines were developed by the ASBS to ensure proper patient selection for this technique.
The ASBS published the outcomes of insertion techniques in a registry trial of 1,403 patients who received MammoSite breast brachytherapy. The trial, initiated in May 2002 by the manufacturer (who relinquished control of the trial in November 2003), accrued patients from 87 institutions over 30 months. Patients were enrolled per the ABS eligibility criteria listed earlier. A total of 1,237 patients (87%) received APBI via MammoSite, 43 (3%) received a boost via MammoSite, and 123 (9%) underwent catheter explantation. Explantation was performed because of poor skin spacing (35%), irregular cavity (28%), positive margins (9%), and balloon failure (9%). A subset analysis of 198 patients with ductal carcinoma in situ with a median follow-up of 15 months was presented at the ASTRO annual meeting in November 2006.These patients received 34.0 Gy in 10 fractions over 5 days. They reported a 1% (n = 1) 2-year actuarial rate of ipsilateral breast tumor recurrence. At 6, 12, 24, and 36 months, the cosmetic results were reported as good or excellent in 94% (n = 180), 97% (n = 103), 89% (n = 28), and 90% (n = 10) of patients. They found that skin spacing greater than 6 mm, larger balloon-to-skin distance, and closed cavity placement were all associated with a good/excellent cosmetic result. Infection occurred in 7% of patients and did not reach statistical significance in terms of cosmetic outcome. At the ASTRO annual meeting in November 2006, Cuttino et al presented a pooled analysis of patients with stage 0, I, and II breast carcinoma treated with MammoSite at nine institutions between 2000 and 2004. All 483 patients received 34 Gy in 10 fractions over 5 days. The median follow-up was 2 years, and all patients had a minimum follow-up of 1 year. They found an in-breast failure rate of 1.2% (n = 6), but only 0.4% of all patients experienced a failure that was characterized as a true recurrence or marginal miss. Cosmetic results were reported as good/excellent in 91% of patients. Administration of prophylactic antibiotics, skin spacing > 5 mm, and use of multiple dwell positions contributed to less dermatologic toxicity in terms of severe acute skin reactions, severe hyperpigmentation, and grade 3/4 acute skin reactions, respectively. A multi-institutional phase II clinical trial was conducted between May 2003 and January 2006 to evaluate the utility of MammoSite in patients with ductal carcinoma in situ.Eligibility criteria included the following: age ≥ 45 years, unicentric pure DCIS, ≥ 1-mm margins, tumor size ≤ 5 cm, clinically node-negative, and a postlumpectomy mammogram showing complete resolution of any suspicious microcalcifications. A total of 133 patients were enrolled, 117 of whom received the MammoSite implant. Seventeen patients underwent removal of the implant for various reasons, including suboptimal skin distance, positive margins, and irregular cavity. Thus, 100 patients completed treatment, with a median follow-up period of 9 months. Two patients experienced an ipsilateral breast recurrence, with one being a true recurrence/marginal miss. Approximately 98% of patients reported a good/excellent cosmetic result, and the researchers found a 4% infection rate, consistent with other series. Details of these studies can be found in Table 3.
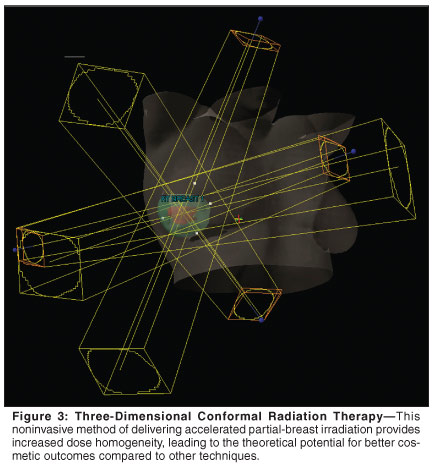
3D Conformal External-Beam Radiotherapy Although the most widely used form of radiation therapy to treat carcinomas of all types, this technique is associated with the least amount of data supporting its role in APBI. Three-dimensional conformal EBRT (3D-CRT) is a noninvasive method of delivering APBI that provides increased dose homogeneity, leading to the theoretical potential for better cosmetic outcomes compared to other techniques (Figure 3). Furthermore, 3D-CRT is less operator-dependent than interstitial brachytherapy and patients do not have to undergo explantation of brachytherapy catheters, as do a proportion of patients treated with MammoSite. In addition, cost-analysis investigations have indicated that 3D-CRT may be less expensive than brachytherapy techniques that do not require an extra surgical procedure or inpatient hospitalization. With the emergence of computed tomography (CT)-based simulation, easier identification of the tumor bed and decreased doses to critical normal structures (in addition to the above reasons) have led to an interest in delivering APBI using 3D-CRT.
• William Beaumont Hospital Study—Vicini and colleagues at the William Beaumont Hospital first used 3D-CRT to deliver APBI in a select group of patients using active breathing control to account for movement of the breast secondary to respiration. They found this technique to be feasible and initiated a phase I/II trial further investigating the role of 3D-CRT in patients who met the eligibility criteria for RTOG 95-17. Thirty-one patients were enrolled and underwent CT-based planning. The clinical target volume (CTV) was defined as the lumpectomy cavity plus a 1- to 1.5-cm margin, limited by the skin surface and chest wall. A 1-cm margin was added to form the planning-target volume (PTV). The first five patients received 34 Gy over 10 twice-daily fractions, while the remainder received 38.5 Gy over 10 twice-daily fractions. With a median follow-up of 10 months, the study revealed no recurrences and a 100% rating of good/excellent cosmesis. The technical aspects of this study were found to be feasible and easily reproducible. • RTOG Study—The RTOG conducted a phase I/II trial to evaluate the feasibility and reproducibility of 3D-CRT in delivering APBI. They enrolled 58 patients with stage I or II invasive ductal carcinoma involving lesions ≤ 3 cm and negative surgical margins. After lumpectomy, the surgical cavity was defined on CT scan, and this was denoted as the gross tumor volume (GTV). An expansion of 1.0 to 1.5 cm was added to form the CTV. The CTV was restricted to within 5 mm of the skin surface and lung-chest wall interface. An additional margin of > 1.0 cm was provided to calculate the PTV, to account for penumbra. However, a separate PTV structure was defined to exclude this volume to within 5 mm of the skin surface and lung-chest wall interface and was used for the dose-volume histogram (DVH) analysis. A total of 38.5 Gy was delivered in 10 fractions over 5 days. Patients were not treated using active breathing control. Port films and orthogonal pair films were taken four times during the course of therapy. The dose-volume constraints were as follows: < 50% of the ipsilateral breast should receive < 50% of the prescribed dose and 25% of the ipsilateral whole breast should receive the prescribed dose; the contralateral breast received < 3% of the prescribed dose; < 10% of the ipsilateral lung could receive 30% of the prescribed dose; < 10% of the contralateral lung could receive 5% of the prescribed dose; < 5% of the heart could receive a maximum of 5% of the prescribed dose for right-sided lesions, and for left sided lesions, the volume of lung receiving 5% of the dose should be less than conventional WBI. Finally, the maximum dose to the thyroid could be 3% of the prescribed dose. The primary endpoint of the study was to determine whether 3D-CRT was reproducible. Indeed, the investigators confirmed the technique's, as there were only four cases with major variations in the first 42 evaluable plans. All four of these major variations arose from the strict DVH constraints on the ipsilateral lung. The results of this study served as the foundation for the external-beam arm of the NSABP B-39/RTOG 0413 clinical trial that opened in 2005. Sequencing With Chemotherapy Systemic therapy has been shown to have a favorable impact on local control in combination with radio-therapy following breast-conservation surgery. Several randomized and retrospective studies have shown a significant decrease in local control in patients treated with lumpectomy followed by a course of systemic therapy and radiotherapy. Although the impact of systemic therapy on local control has been proven, how best to implement systemic therapy with respect to radiation therapy is debatable. With current chemotherapeutic regimens for treating invasive breast cancer, the use of concurrent radiotherapy is discouraged as side effects are significantly increased. A meta-analysis investigating the sequencing of adjuvant radiotherapy and chemotherapy in breast cancer revealed a significant increase in 5-year locoregional recurrence rates—from 5.8% in patients treated with radiotherapy within 8 weeks of surgery, to 9.1% in patients receiving treatment between 9 and 16 weeks after surgery. However, a prospective study by Bellon et al told a different story. Patients were randomized to 12 weeks of chemotherapy (cyclophosphamide, doxorubicin, methotrexate, fluorouracil, and prednisone) before or after WBI. Even though no difference in local control, distant metastases, or overall survival was identified, a relationship between local control, margin status, and sequencing was shown. Patients with negative margins had a local recurrence rate of 6% in the chemotherapy-first group and 13% in the radiotherapy-first group. In patients with close margins, the local recurrence rate was 32% in the chemotherapy-first group and 4% in the radiotherapy-first group. Several studies investigating the role of concurrent chemotherapy and radiation therapy showed significant reductions in local recurrence rates. However, these studies used older chemotherapeutic regimens. • Impact of APBI on Sequencing—With APBI, radiotherapy may be delivered earlier in the course of treatment. Given the short course of treatment, APBI may be sandwiched between surgery and chemotherapy, essentially dissolving the debate about sequencing of radiotherapy with chemotherapy. The NSABP/RTOG study investigating APBI in early-stage breast cancer patients mandates that patients randomized to APBI who are recommended for chemotherapy receive radiotherapy prior to any chemotherapy administration. Single-institution experiences from two different groups found that patients who received HDR interstitial brachytherapy followed by anthracycline-based regimens experienced increased complications of varying types. A group led by David Wazer found that 50% of these patients experienced fat necrosis, compared to 19% of patients who did not receive chemotherapy. The investigators found a higher incidence of ≥ grade 2 subcutaneous toxicity and a lower rate of excellent cosmetic results. A study by Arthur et al demonstrated a striking increase of radiation recall in doxorubicin-treated patients, which continued with varying intensity during each subsequent cycle of chemotherapy. Interestingly, this group concluded that LDR brachytherapy was associated with poorer cosmetic outcome when preceding doxorubicin. A pilot study presented by Johns Hopkins University researchers at the ASTRO annual meeting in November 2006 evaluated APBI concurrent with dose-dense doxorubicin and cyclophosphamide (ddAC). They enrolled women with T1-2, N0-1 invasive breast carcinoma status postlumpectomy with negative margins to receive ddAC (60 and 600 mg/m2, respectively) every 14 days with growth factor support. The radiation was delivered to the tumor bed plus margin in 2.7-Gy fractions over 15 fractions to a total dose of 40.5 Gy. Radiotherapy was started within 2 days of the first chemotherapy dose. With 13 patients treated and a median follow-up of 9 months, they reported no radiation recall and no radiation dermatitis greater than grade 1. Moreover, they reported no signs of late skin or soft-tissue toxicity. Although these results are preliminary and encouraging, they do raise questions about determining the optimal timing and dose-fractionation schema of APBI in relation to chemotherapy. In an analysis of the ASBS MammoSite registry trial, Haffty et al recently reported that following MammoSite brachytherapy, cosmetic outcome appeared to be superior in patients whose chemotherapy was initiated more than 3 weeks after the last MammoSite brachytherapy procedure. Cosmetic outcome was good to excellent in 94% of women receiving chemotherapy later than 3 weeks after the last procedure, compared to 83% good-to-excellent cosmesis in women receiving chemotherapy within 3 weeks of the last MammoSite procedure (P = .09). Of note, the cosmetic outcome in women receiving chemotherapy more than 3 weeks after the procedure was similar to the cosmetic outcome of the overall population not receiving chemotherapy. Longer follow-up and additional data will be required to determine the optimal timing of chemotherapy following APBI with the various techniques employed. Research is still needed to help determine the optimal dose per fraction, timing with chemotherapy, and treatment of patients with adverse risk factors. To date, results from the phase I/II studies discussed above are encouraging and may lead to a shift in the treatment paradigm in early-stage breast cancer patients. Only through the enrollment of patients on these ongoing randomized clinical trials, and through development of novel phase I/II programs evaluating other issues related to fractionation, positioning, and techniques, can we continue to move forward with this rapidly evolving field of accelerated partial-breast irradiation. • NYU Study—Formenti and colleagues at New York University designed a phase I/II study in 2000 evaluating the role of APBI delivered, using 3D-CRT, to patients laying in the prone position. Advocates of this approach maintain that the prone position reduces normal tissue motion secondary to respiration and cardiac systole, and further allows for the removal of the heart and lungs from the treatment field. This group treated 78 patients with a median follow-up of 28 months—the longest follow-up of APBI using 3D-CRT to date. As of this writing, there have been no recurrences, and cosmesis was rated as good/excellent in 92% of patients. Details on the experience with 3D-CRT are listed in Table 4.
|