|
|
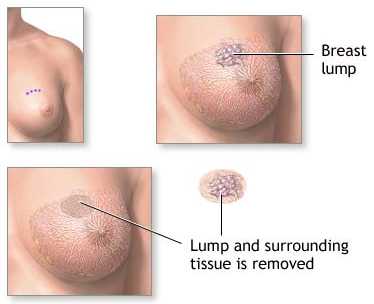
Surgical
Margins and Lumpectomy |
|
|
Surgical
Margins and Lumpectomy |
| The recommended technique states that "The assessment of surgical margins is arguably the most important aspect in the pathologic evaluation of breast tumor excision in patients being considered for breast conservation. Although the definitions of "positive" and "negative" margins vary among institutions, microscopic margin involvement appears to be associated with an increased risk of local recurrence and, usually, indicates a need for further surgery, such as reexcision of the tumor site" We prefer to have clear margins before starting radiation, but additional surgery if it requires removal of large amounts of tissue or another anesthesia may not be absolutely necessary, if the margin involved was minor (or focal.) As noted in the literature below this area remains controversial. Since the radiation technique includes radiation to the whole breast followed by an extra 'boost' doe to the lumpectomy site, the radiation may be able to sterilize the cancer in most patients, though we generally would assume the risk of a local relapse is a bit higher with + margins, the impact on overall survival may be minimal as in the recent study of U of Penn on 1,021 cases ( Peterson IJROBP 1999;43:1029) |
| margin: | negative marg. | positive marg. | close marg. |
| local relapse | 8% | 10% | 17% |
| survival/8 years | 86% | 83% | 88% |
Patients should understand that when further surgery is done because of positive margins, cancer is not always found, In one literature review (Morrow IJROBP 1996:34:1173) if the initial margins were negative cancer was found in 25-48% of the resected tissue and if the margins were positive cancer was found in 42-69%. In other words some women who will opt to have a mastectomy because the original biopsy showed cancer at the margins, will be found to have no cancer in the resected breast.. The risk of relapse in the breast varies considerably in different studies, based on the margins as noted in the review by Smitt. Cancer 1995;76:259 below: |
| negative margin | 2 - 10% |
| indeterminate margin | 7 - 15% |
| positive margin | 8 - 22% |
Its worth noting that even with positive margins if the patient is given 'boost radiation (an extra dose at the lumpectomy site) the local relapse may be as low as those with negative margins as noted below from Cancer 1996;78:1728 |
| margins negative | margins positive | |
| Boost XRT | 2-7% | 2-22% |
| No Boost XRT | 2-10% | 12-30% |
It is also worth noting that chemotherapy improves the local control in these patients. In one study of patients with positive margins local control was only 86% but if they received chemotherapy along with the radiation local control 98%. (Smitt. Cancer 1995;76:259.) See the Studies Below:
Ann Surg 1993 Jul;218(1):22-8 Local failure and margin status in early-stage breast carcinoma treated with conservation surgery and radiation therapy.Anscher Duke University The optimal extent of breast surgery required for patients treated with conservation surgery and radiation therapy has not been established. To achieve breast preservation with good cosmesis, it is desirable to resect as little normal tissue as possible. However, it is critical that the resection does not leave behind a tumor burden that cannot be adequately managed by moderate doses of radiation. It is not known whether microscopically positive surgical margins are detrimental to patient outcome. METHODS: The records of 259 consecutive women (262 breasts) treated with local excision (complete removal of gross tumor with a margin) and axillary dissection followed by radiation therapy for clinical stage I and II infiltrating ductal breast cancer at Duke University Medical Center and the University of North Carolina between 1983 and 1988 were reviewed. Surgical margins were considered positive if tumor extended to the inked margins; otherwise the margins were considered negative. Of the 262 tumors, 32 (12%) had positive margins, 132 (50%) had negative margins, and the remaining 98 (38%) had indeterminate margins. There were 11 (4%) local failures; 3/32 (9%) from the positive margin group, 2/132 (1.5%) from the negative margin group, and 6/98 (6%) from the indeterminate group. The actuarial local failure rates at 5 years were 10%, 2%, and 10%, respectively, p = 0.014 positive vs. negative, p = 0.08 positive vs. indeterminate (log rank test). Margin status had no impact on survival or freedom from distant metastasis; 63 patients who originally had positive or indeterminate margins were re-excised. Two of 7 with positive margins after re-excision versus 1/56 rendered margin negative had a local recurrence. CONCLUSIONS: The authors recommend re-excision for patients with positive margins because of improved local control of those rendered margin negative and identification of those patients at high risk for local failure (those who remain positive after re-excision). Because margin status impacts on local control, tumor margins after conservation surgery should be accurately determined in all patients. Ann Oncol 1999 Dec;10(12):1451-5 Local relapse in primary breast cancer patients with unexcised positive surgical margins after lumpectomy, radiotherapy and chemoendocrine therapy.Assersohn.Royal Marsden Hospital, Surrey, UK. Inadequate surgical excision with residual involvement of resection margins by tumour after breast conservation results in increased local recurrence rates. To reduce this risk positive margins are, therefore, usually excised. Systemic treatment with tamoxifen or chemotherapy reduces local recurrence, along with radiotherapy. Histological resection margin was considered positive if ductal carcinoma in situ (DCIS) or invasive carcinoma was present microscopically less than 1 mm from the excision margin. RESULTS: Although 38% of patients had unexcised microscopically involved margins, local relapse rate as first site of relapse was only 1.9% after a median follow up of 57 months. There was no difference in distant relapse (P = 0.2) and survival (P = 0.5) between the positive and negative margins groups. CONCLUSIONS: The presence of positive unexcised margins does not have a significant effect on outcome in patients who are treated with chemoendocrine therapy together with radiotherapy. Further clinical trials are required. Cancer 1998 Jun 1;82(11):2212-20 The number of positive margins influences the outcome of women treated with breast preservation for early stage breast carcinoma.DiBiase Jefferson Medical College, There are conflicting reports regarding whether
focally positive surgical margins influence tumor control in breast-conservation therapy.
Patients underwent excisional biopsy and margin sampling with shaved biopsies of the tumor
cavity. The entire breast received 45 grays (Gy) with a 20-Gy iridium-192 implant or an
electron boost. Eighty-six patients had microscopically positive margins (19%), and the
remainder had confirmed negative margins. Local tumor control rates for patients with
negative margins at 5 and 10 years were 94% and 87%, respectively, compared with 86% and
69%, respectively, for those patients with positive margins (P=0.005). The disease free
survival rates for the negative margin group at 5 and 10 years were 91% and 82%,
respectively, compared with 76% and 71%, respectively, for the positive margin group
(P=0.001). Overall survival rates for patients with negative margins at 5 and 10 years
were 95% and 84%, respectively, compared with 87% and 78%, respectively, for those with
positive margins (P=0.047). When comparing the negative margin group with the one positive
margin group, there was no significant difference in local tumor control (P=0.12).
However, women with two or more positive margins had an inferior local tumor control
compared with those women with negative margins (P=0.002). CONCLUSIONS: Patients with
positive margins have a higher risk for local failure and worse survival when undergoing
breast conservation therapy. Inferior local tumor control was noted in those patients with
two or more positive margins. Int J Radiat Oncol Biol Phys 1996 Mar 15;34(5):1009-17 Does the placement of surgical clips within the excision cavity influence local control for patients treated with breast-conserving surgery and irradiation.Fein Fox Chase Center A number of authors have demonstrated the
importance of using surgical clips to define the tumor bed in the treatment planning of
early-stage breast cancer. The clips have been useful in delineating the borders of the
tangential fields, especially for very medial and very lateral lesions as the boost
volume. If surgical clips better define the tumor bed, then a reduction in true or
marginal recurrences should be appreciated. We sought to compare the incidence of breast
recurrence in women with and without surgical clips, controlling for other recognized
prognostic factors. The actuarial probability of a breast recurrence was 2% at 5
years and 5% at 10 years for patients without clips compared to 5 and 11%, respectively,
for patients with clips (p=0.01). Overall, there was a significant difference in the
10-year breast recurrence rate favoring women without clips despite more adverse
prognostic factors. There was no difference in the breast recurrence rate for patients
with or without surgical clips if careful attention to margin status was addressed.
Failure to ink the surgical specimen resulting in unknown margins cannot be compensated
for with the placement of . Int J Radiat Oncol Biol Phys 1999 Jul 15;44(5):1005-15 Patients with early stage invasive cancer with close or positive margins treated with conservative surgery and radiation have an increased risk of breast recurrence that is delayed by adjuvant systemic therapy.Freedman Fox Chase The association between a positive resection
margin and the risk of ipsilateral breast tumor recurrence (IBTR) after conservative
surgery and radiation is controversial. The width of the resection margin that minimizes
the risk of IBTR is unknown. While adjuvant systemic therapy may decrease the risk of an
IBTR in all patients, its impact on patients with positive or close margins is largely
unknown. This study examines the interaction between margin status, margin width, and
adjuvant systemic therapy on the 5- and 10-year risk of IBTR after conservative surgery
and radiation. The final margins were negative in 77%, positive in 12%, and close (< or
= 2 mm) in 11%. The median total dose to the tumor bed was 60 Gy with negative margins, 64
Gy with close margins, and 66 Gy with positive margins. Chemotherapy +/- tamoxifen was
used in 28%, tamoxifen alone in 20%, and no adjuvant systemic therapy in 52%. RESULTS: The
5-year cumulative incidence (CI) of IBTR was not significantly different between patients
with negative (4%), positive (5%), or close (7%) margins. However, by 10 years, a
significant difference in IBTR became apparent (negative 7%, positive 12%, close 14%, p =
0.04). There was no significant difference in IBTR when a close or positive margin was
involved by invasive tumor or DCIS. Reexcision diminished the IBTR rate to 7% at 10 years
if the final margin was negative; however, the highest risk was observed in patients with
persistently positive (13%) or close (21%) (p = 0.02) margins. The median interval to
failure was 3.7 years after no adjuvant systemic therapy, 5.0 years after chemotherapy +/-
tamoxifen, and 6.7 years after tamoxifen alone. This delay to IBTR was observed in
patients with close or positive margins, with little impact on the time to failure in
patients with negative margins. The 5-year CI of IBTR in patients with close or positive
margins was 1% with adjuvant systemic therapy and 13% with no adjuvant therapy. However,
by 10 years, the CI of IBTR was similar (18% vs. 14%) due to more late failures in the
patients who received adjuvant systemic therapy. CONCLUSION: A negative margin (> 2 mm)
identifies patients with a very low risk of IBTR (7% at 10 years) after conservative
surgery and radiation. Patients with a close margin (< or = 2 mm) are at an equal or
greater risk of IBTR as with a positive margin, especially following a reexcision. A
margin involved by DCIS or invasive tumor has the same increased risk of IBTR. A
reexcision of an initially close or positive margin that results in a negative final
margin reduces the risk of IBTR to that of an initially negative margin. A close or
positive margin is associated with an increased risk of IBTR even in patients who are
EIC-negative or receiving higher boost doses of radiation. The median time to IBTR is
delayed; however, the CI is not significantly decreased by adjuvant systemic therapy in
patients with close or positive margins-the 5 year results in these patients underestimate
their ultimate risk of recurrence. Cancer 1996 Nov 1;78(9):1921-8 Pathologic margin involvement and the risk of recurrence in patients treated with breast-conserving therapy.Gage I, Schnitt Harvard, Medical School The relationship between the microscopic margins of resection and ipsilateral breast
recurrence (IBR) after breast-conserving therapy for carcinomas with or without an
extensive intraductal component (EIC) has not been adequately defined. Final inked
margins of excision were classified as negative > 1 mm (no invasive or in situ ductal
carcinoma within 1 mm of the inked margin); negative-1 mm, or close carcinoma < or = 1
mm from the inked margin but not at the margin); or positive (carcinoma at the inked
margin). A focally positive margin was defined as invasive or in situ ductal carcinoma at
the margin in three or fewer low-power fields. The first site of recurrent disease was
classified as either ipsilateral breast recurrence (IBR) or distant metastasis/regional
lymph node failure. The 5-year rate of IBR for all patients with negative margins was 2%;
and for all patients with positive margins, the rate was 16%. Among patients with negative
margins, the 5-year rate of IBR was 2% for all patients with close margins (negative <
or = 1 mm) and 3% for those with negative > 1 mm margins. For patients with close
margins, the rates were 2% and 0% for EIC-negative and EIC-positive tumors, respectively;
the corresponding rates for patients with negative margins > 1 mm were 1% and 14%. The
5-year rate of IBR for patients with focally positive margins was 9% (9% for EIC-negative
and 7% for EIC-positive patients). The 5-year crude rate of IBR for patients with greater
than focally positive margins was 28% (19% for EIC-negative and 42% for EIC-positive
patients). CONCLUSIONS: Patients with negative margins of excision have a low rate of
recurrence in the treated breast, whether the margin is > 1 mm or < or = 1 mm and
whether the carcinoma is EIC-negative or EIC-positive. Among patients with positive
margins, those with focally positive margins have a considerably lower risk of local
recurrence than those with more than focally positive margins, and could be considered for
breast-conserving therapy. Int J Radiat Oncol Biol Phys 1999 Mar 15;43(5):1029-35 Outcomes in breast cancer patients relative to margin status after treatment with breast-conserving surgery and radiation therapy: the University of Pennsylvania experience.Peterson University of Pennsylvania To evaluate the significance of final microscopic resection margin status on treatment
outcomes in women with early breast cancer who are treated with breast-conserving surgery
and definitive breast irradiation. The 1021 patients were divided into four groups based
on the final microscopic margin from the tumor excision or from the re-excision if
performed. These four groups were: (a) 518 patients with negative margins; (b) 124
patients with focally positive margins; (c) 96 patients with focally close margins (<
or = 2 mm); and (d) 283 patients with unknown margins. RESULTS: Local failure was not
significantly different in patients with negative, focally positive, focally close or
unknown final pathologic margins of resection at 8 years (8% vs. 10% vs. 17% vs. 16%,
respectively, p = 0.21). The 8-year outcome also was not different among the four groups
for overall survival (86% vs. 83% vs. 88% vs. 81%, respectively, p = 0.13), cause-specific
survival (89% vs. 86% vs. 88% vs. 83%, respectively, p = 0.14), no evidence of disease
survival (81% vs. 73% vs. 86% vs. 77%, respectively, p = 0.09), and freedom from distant
metastases (85% vs. 75% vs. 86% vs. 79%, respectively, p = 0.08). CONCLUSION: These
results demonstrate that selected patients with focally positive or focally close
microscopic resection margins can be treated with breast-conserving surgery and definitive
breast irradiation with 8-year local control rates and survival rates that are similar to
those seen in breast-conservation patients with negative or unknown final resection
margins. Surgery 1994 Oct;116(4):605-8; discussion 608-9 Importance of margin status in outcome of breast-conserving surgery for carcinoma.Pittinger University of Rochester Two hundred eleven patients were classified based on initial margin status: negative
(more than 3 mm), close (3 mm or less), positive, or unknown. The incidence of reexcision
and residual tumor is reported in each group. Patients with 36 months or more of follow-up
(n = 183) were also stratified by final margin to examine rates of local recurrence and
distant recurrence. RESULTS. Residual carcinoma was found in 0%, 24%, 44%, and 48% of the
negative, close, positive, and unknown initial margin groups, respectively. The local
recurrence rate was equivalent by Fisher exact test in patients with negative and close
final margins (3%). The negative and close groups were not different by chi-squared
analysis in terms of T stage, estrogen receptor status, and nodal status. CONCLUSIONS.
Although one fourth of patients with close margins have residual tumor, recurrence rates
are similar to those with negative margins. Reexcision of close margins is not necessary
in patients who undergo BCT for carcinoma. Cancer 1994 Sep 15;74(6):1746-51 The relationship between microscopic margins of resection and the risk of local recurrence in patients with breast cancer treated with breast-conserving surgery and radiation therapy.Schnitt Beth Israel Hospital, Boston BACKGROUND. The relationships among the involvement of tumor at the final margins of
resection, the presence of an extensive intraductal component (EIC), and the risk of local
recurrence are important considerations in patients treated with conservative surgery and
radiation therapy for early stage breast cancer but have not been defined adequately. A
positive margin was defined as tumor present at the inked margin of resection, a close
margin as tumor within 1 mm of the inked margin, and a negative margin as no tumor within
1 mm of the inked margin. A focally positive margin was defined as tumor at the margin in
three or fewer low-power fields. In 157 patients (87%), the tumor was evaluable for the
presence or absence of an EIC. The median follow-up was 86 months. In 12 of 181
patients (7%), a recurrence developed at or near the primary site (true
recurrence/marginal miss [TR/MM]) within 5 years. The 5-year rate of TR/MM (with 95%
confidence intervals) among patients with negative, close, focally positive, and more than
focally positive margins was 0% (0-4%), 4% (0-20%), 6% (1-17%) and 21% (10-37%),
respectively. Patients with positive margins also were more likely to have a distant
failure within 5 years (14%, 8%, 25%, and 32% in the four groups, respectively). However,
patients with positive margins more often had positive axillary lymph nodes than patients
with negative or close margins (59% vs. 38%, P < 0.02). The 5-year rate of TR/MM was
20% for patients with an EIC-positive tumor and 7% for patients with an EIC-negative
tumor. However, among the 127 patients with an EIC-negative tumor, the 5-year rate of
TR/MM was less than 10% in all margin groups. Among the 30 patients with an EIC-positive
tumor, the 5-year rate of TR/MM was 0% when margins were negative or close but 50% when
margins were more than focally positive. CONCLUSIONS. These results provide support for
the use of breast-conserving surgery and breast irradiation in all patients with
uninvolved margins, whether the tumor is EIC-positive or EIC-negative. This study suggests
that breast-conserving therapy (including a radiation boost to the primary site) also may
be a reasonable option for some patients with an EIC-negative tumor and margin
involvement. Cancer 1995 Jul 15;76(2):259-67 The importance of the lumpectomy surgical margin status in long-term results of breast conservation.Smitt Stanford University The surgical margin was classified as positive (transecting the inked margin), close
(less than or equal to 2 mm from the margin), negative, or indeterminate, based on the
initial biopsy findings and reexcision specimens, as appropriate. The actuarial
probability of freedom from local recurrence for the entire group of patients at 5 and 10
years was 94% and 87%, respectively. The actuarial probability of local control at 10
years was 98% for those patients with negative surgical margins versus 82% for all others
(P = 0.007). The local control rate at 10 years was 97% for patients who underwent
reexcision and 84% for those who did not. Reexcision appears to convey a local control
benefit for those patients with close, indeterminate, or positive initial margins, when
negative final margins are attained (P = 0.0001). Final margin status was the most
significant determinant of local recurrence rates in univariate analysis. By multivariate
analysis, the final margin status and use of adjuvant chemotherapy were significant
prognostic factors. CONCLUSIONS. The attainment of negative surgical margins, initially or
at the time of reexcision, is the most significant predictor of local control after
breast-conserving treatment with lumpectomy and radiation therapy. Int J Radiat Oncol Biol Phys 1991 Jul;21(2):279-87 The significance of the pathology margins of the tumor excision on the outcome of patients treated with definitive irradiation for early stage breast cancer.Solin University of Pennsylvania To evaluate the significance of the pathology margins of the tumor excision on the outcome of treatment, an analysis was performed of 697 consecutive women with clinical Stage I or II invasive carcinoma of the breast treated with breast-conserving surgery and definitive irradiation. Complete gross excision of the primary tumor was performed in all cases, and an axillary staging procedure was performed to determine pathologic axillary lymph node status. The 697 patients were divided into four groups based on the final pathology margin from the primary tumor excision or from the re-excision if performed. These four groups were: (a) 257 patients with a negative margin (greater than 2 mm), (b) 57 patients with a positive margin, (c) 37 patients with a close margin (less than or equal to 2 mm), and (d) 346 patients with an unknown margin. The patients with positive final pathology margins were focally positive on microscopic examination. Patients with grossly positive margins or with diffusely positive microscopic margins were treated with conversion to mastectomy. There was a significant difference in the total radiation dose for the four groups (median dose of 6000 vs 6500 vs 6400 vs 6240 cGy, respectively; p less than .0001). There was no significant difference among the four groups for 5-year actuarial overall survival (p = .19), no evidence of disease (NED) survival (p = .95), or relapse-free survival (p = .80). There was no significant difference among the four groups for five year actuarial local or regional control (all p greater than or equal to .29). Subset analyses did not identify any poor outcome subgroups. These results have demonstrated that selected patients with focally positive or close microscopic pathology margins can be adequately treated with definitive breast irradiation. Patient selection and the technical delivery of radiation treatment including a boost may have been important contributing factors to the good outcome in these patients. |
![]()
![]()
![]()
![]()
![]()
![]()
![]()

{kind=link}
{kind=link}