|
|
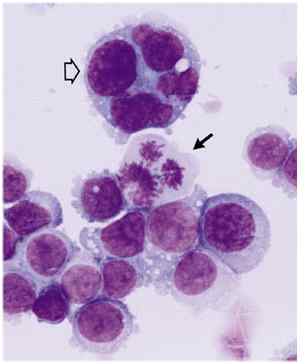
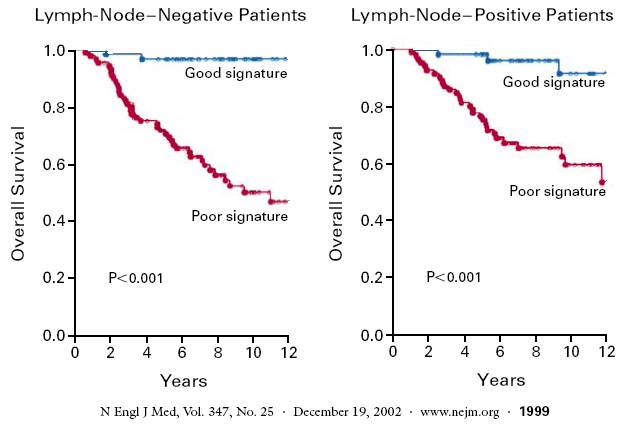
Breast cancer cells start out as normal milk duct cells. The more mutated they become, the more serious and the greater the risk of spread. The degree of abnormality is called the grade (slow growing cells would be low grade or grade 1, medium abnormal would be grade 2 or moderate, and fast growing, very mutated appearing cells would be grade 3 or 4 or high grade or poorly differentiated.) Studies show that higher grade tumors are more likely to relapse (see data.) Some cancers have an abnormal
genetic pattern referred to as over expression or
amplification of HER2 neu and may be treated differently (Herceptin
or Lapatinib) and see section on
Oncotype
Dx below and the discussion on classifying cancer by molecular subgroups (here) Risk of relapse in patients with negative (clear) lymph nodes is related to how mutated the cells are or how rapidly dividing, the risk of relapse in Stage I cancers is as noted below: |
{kind=link}