Anal Cancer |
Anal Cancer |
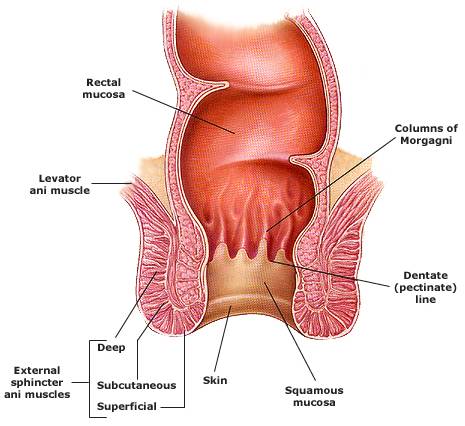 |
The anus consists of a mucosa-lined
anal canal and an epidermis-lined anal margin. The proximal end of the anal canal begins
anatomically at the junction of the puborectalis portion of the levator ani muscle and the
external anal sphincter, and extends distally to the anal verge, a distance of
approximately 4 cm. The anal canal is divided by the dentate line, which overlies the
transition from glandular (columnar) to squamous mucosa that is often referred to as the
transitional zone. The anal margin begins approximately at the anal verge, which
corresponds to the introitus of the anal orifice. It represents the transition from the
squamous mucosa to the epidermis-lined perianal skin, and extends to the perianal skin.
At initial presentation, most patients have a T1 or T2 lesion and fewer than 20 percent are node-positive. In a series of 270 patients with anal canal SCC, the distribution of stage at diagnosis was as follows
In the above series of 270 patients, the five-year survival by stage was
|
|
patients with squamous cell
carcinoma of the anal canal are generally treated with wide
local excision for in-situ cases (if margins are negative) or with
radiation. The more advanced cases get radiation usually combined with
chemotherapy (see NCCN guidelines for anal
canal). Patients with cancer of the anal margin may be
treated with local surgery (see guidelines for
anal margin). Following this, patients are checked every few months
(without biopsy unless there is a suspicious area,
see NCCN follow-up guidelines.) Go
here for NCCN anal site
|


{kind=link}
{kind=link}
{kind=link}
{kind=link}